Man 52 yo, voice tone changes for 2 months, and ENT doctor said vocal
paralysis by endoscopy.
Ultrasound of the neck
US1 left thyroid lobe normal

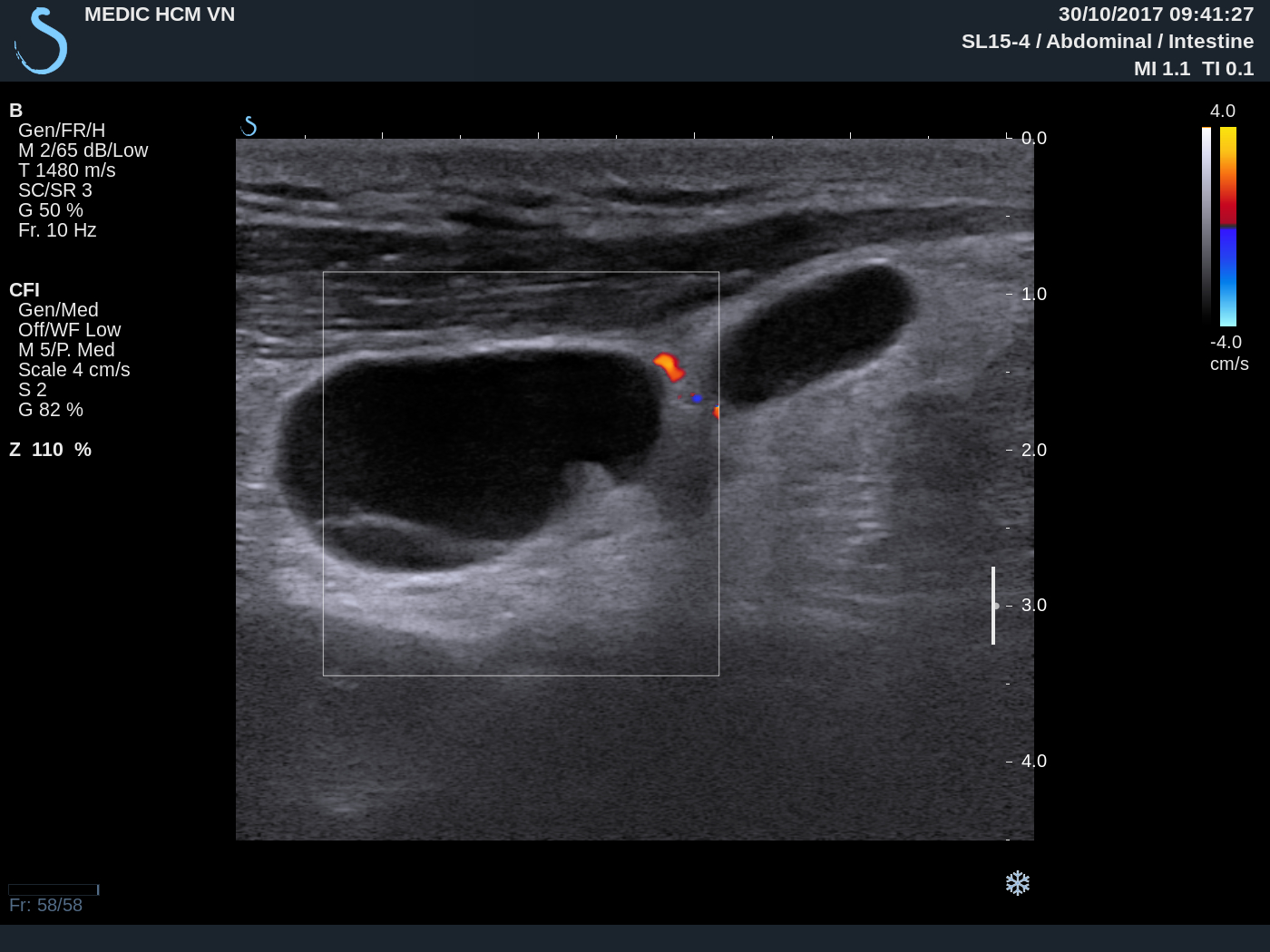
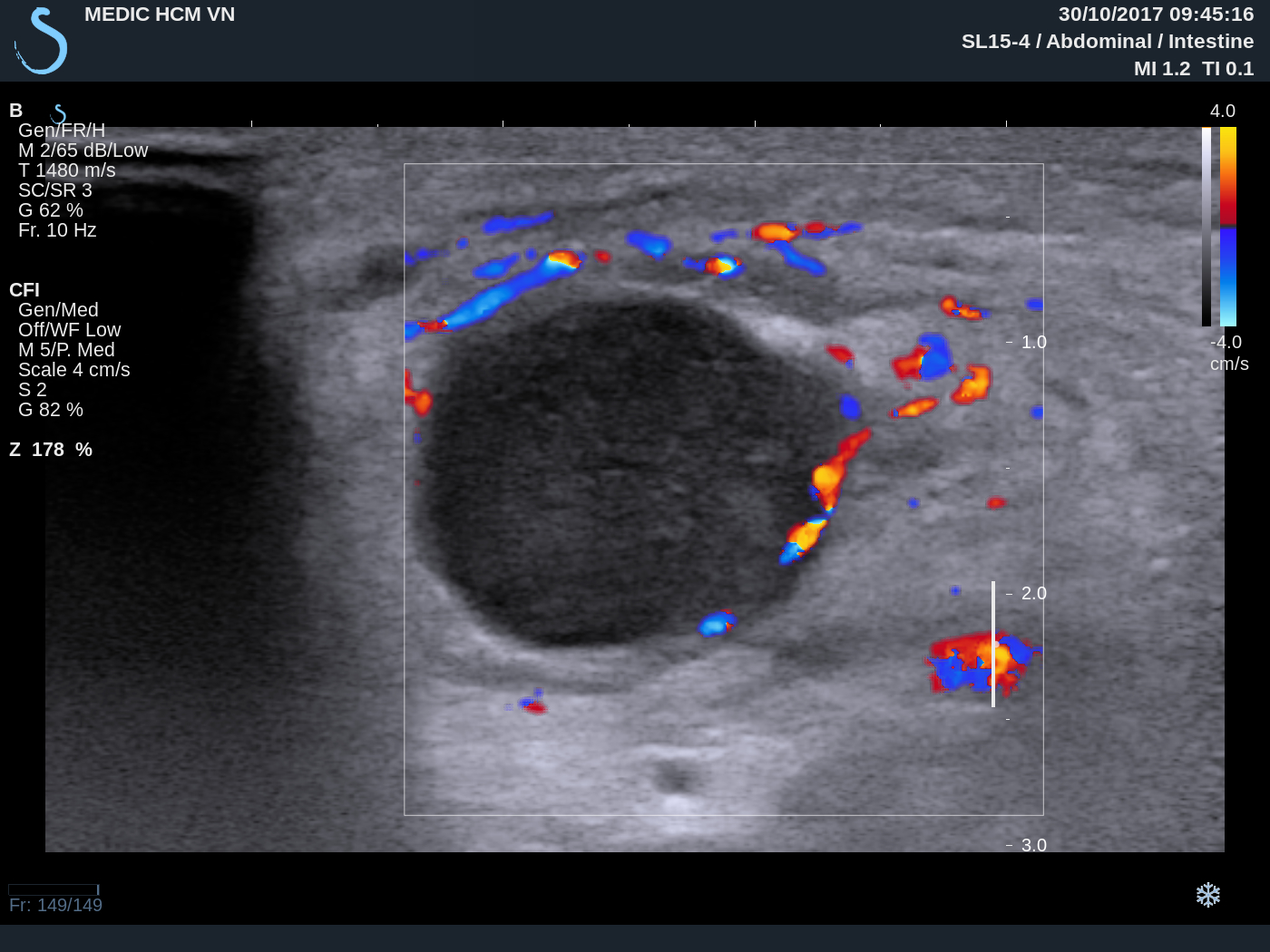
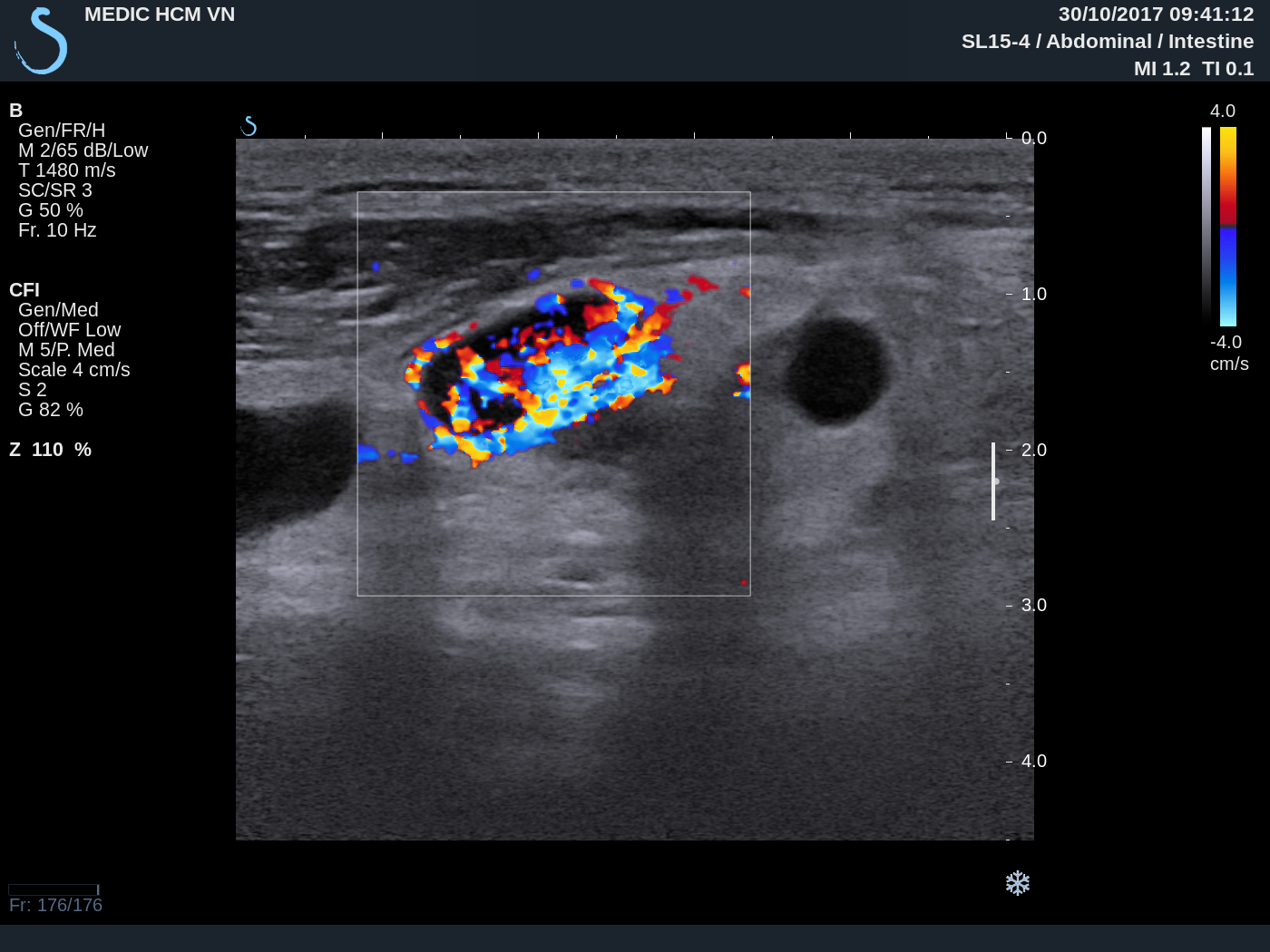
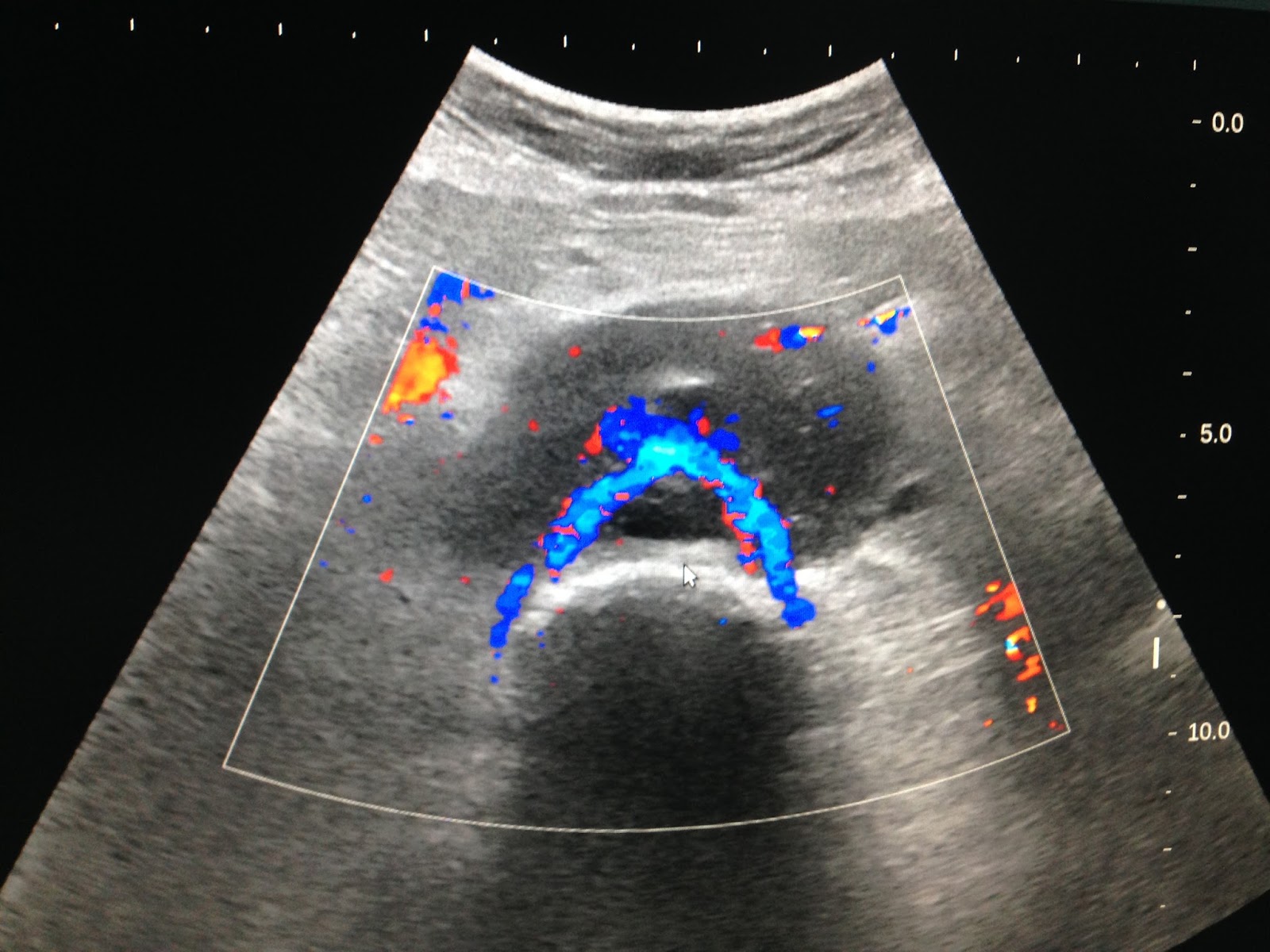
US2 right lobe
covered by a big mass 4 cm with strong posterior shadowing
cannot see structure inside.

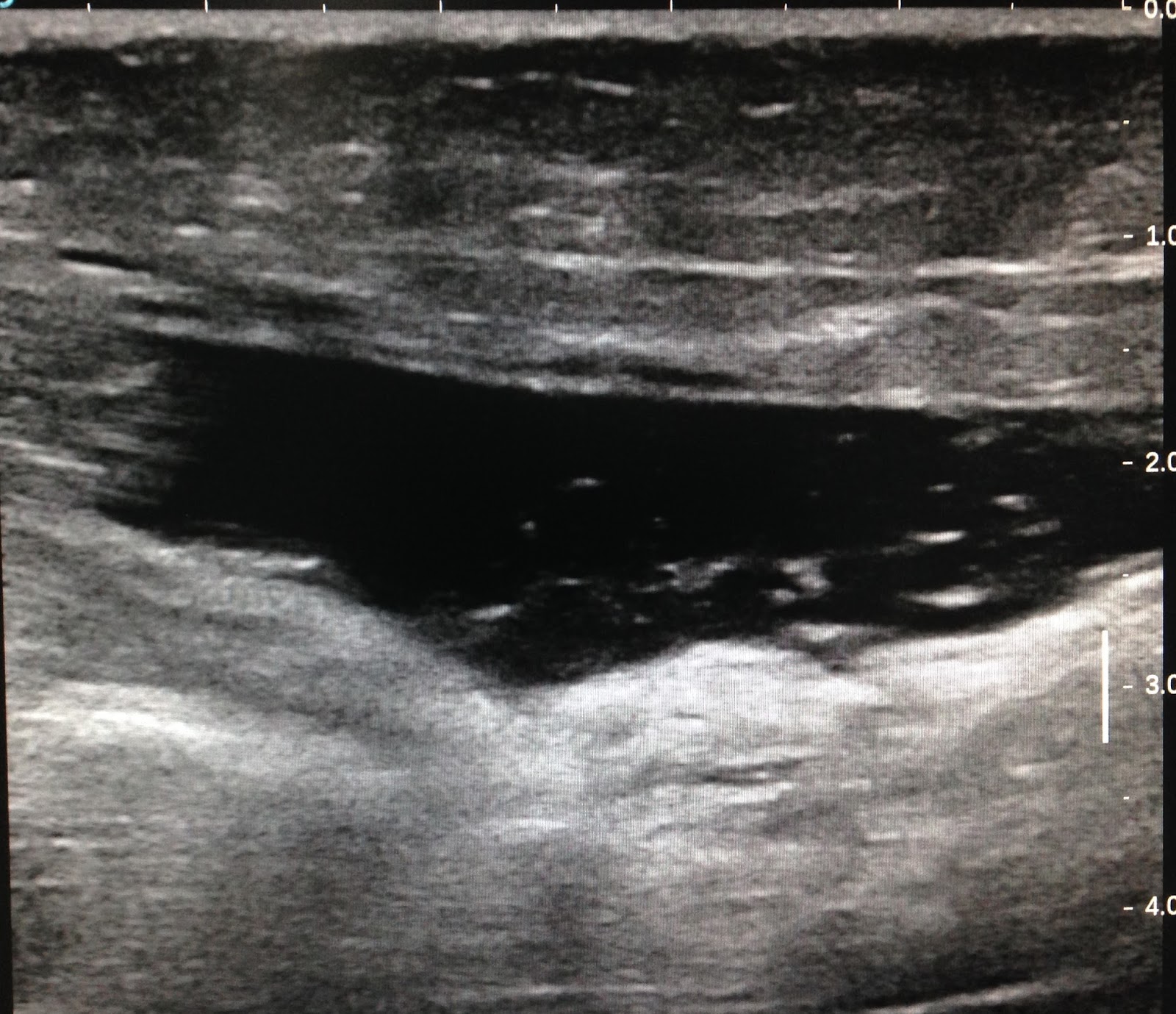
US3 near R/ CCA small nodes with calcification #1cm.

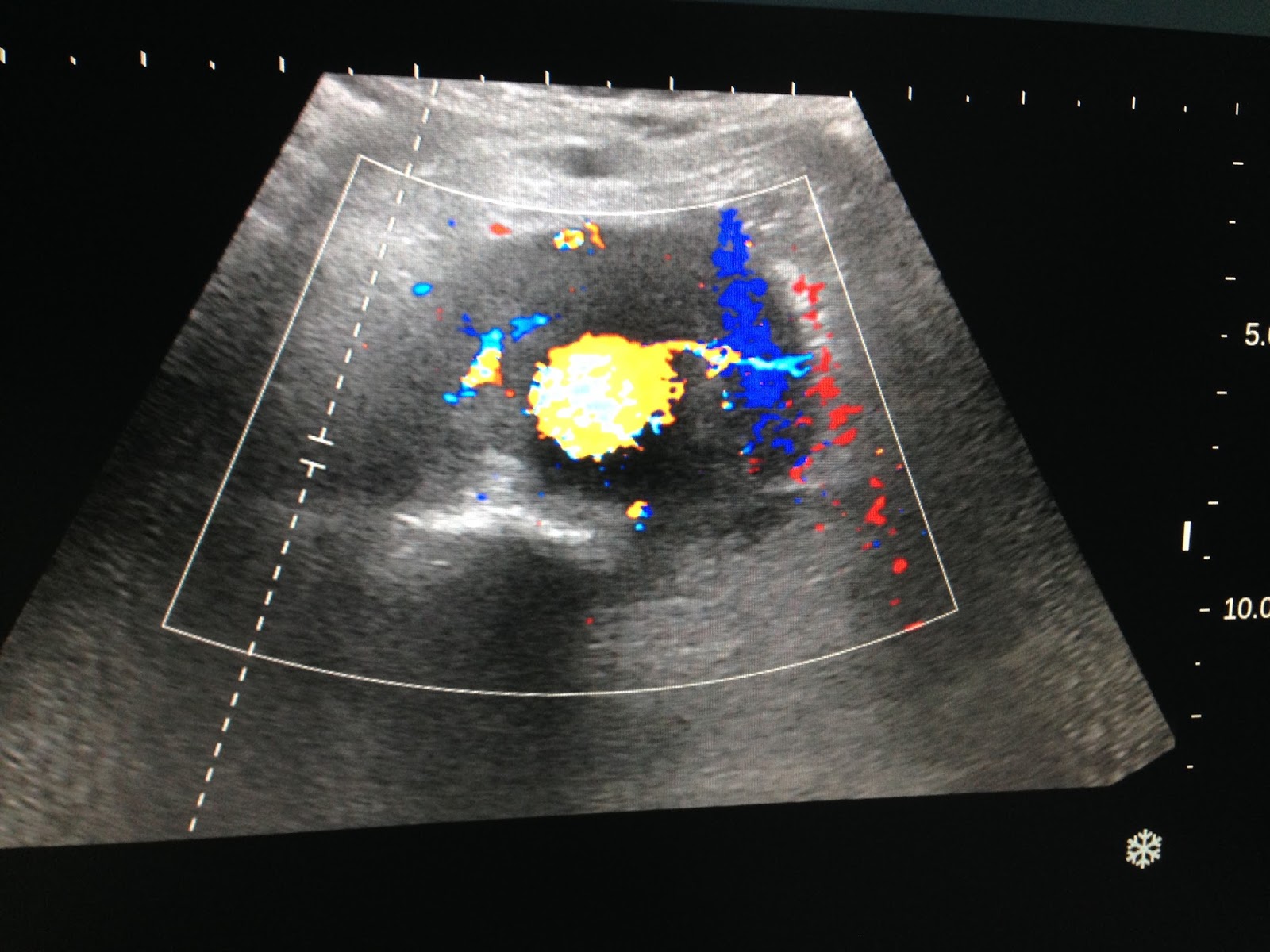
US4 with convex probe ultrasound cannot se intra tumor by
very strong calcification.

MTSC non CE
CT1: cross- section of the neck = mass is very high calcification
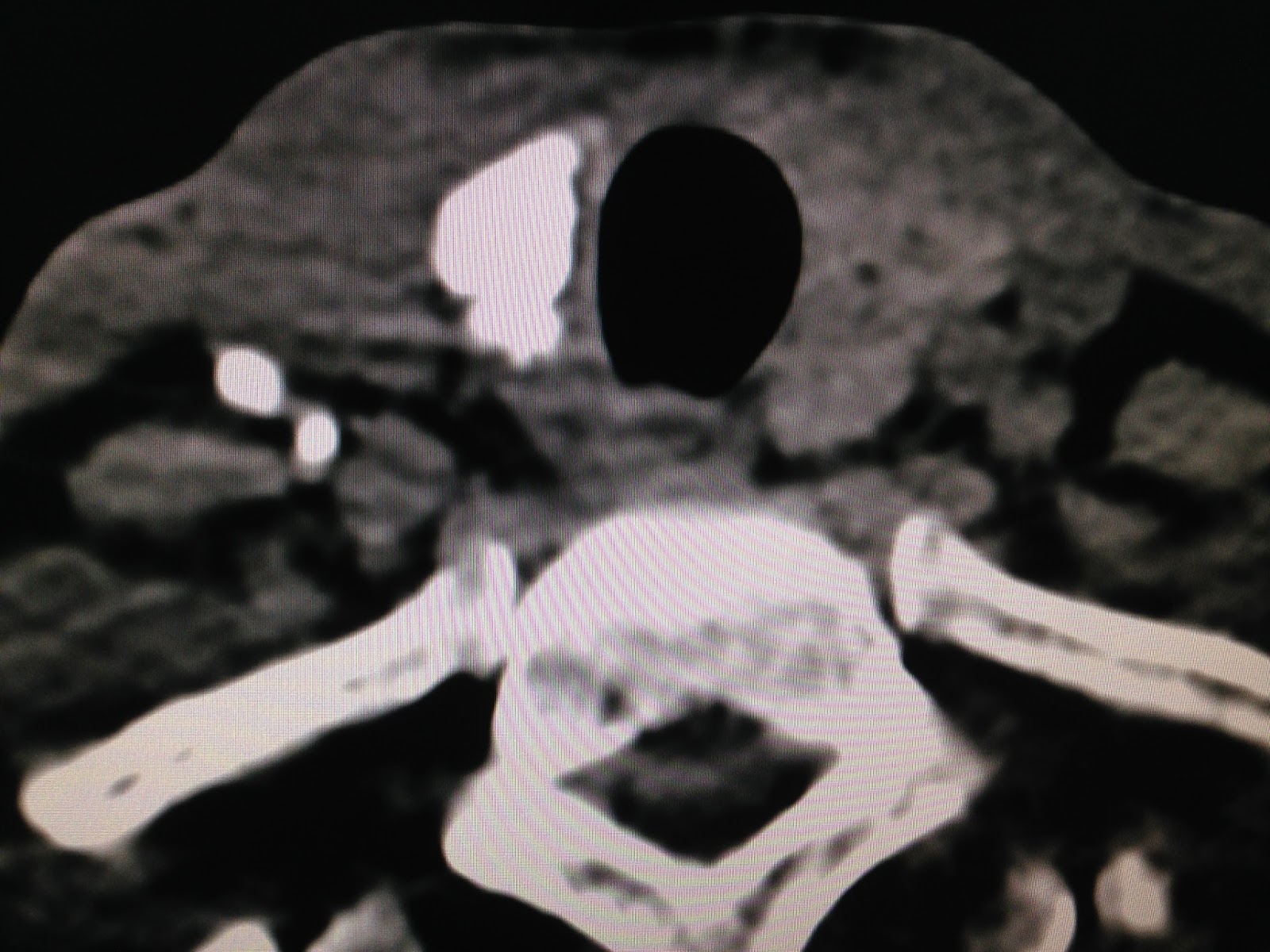
CT2 : cross- section= calcification some lymph nodes
near R/ CCA.

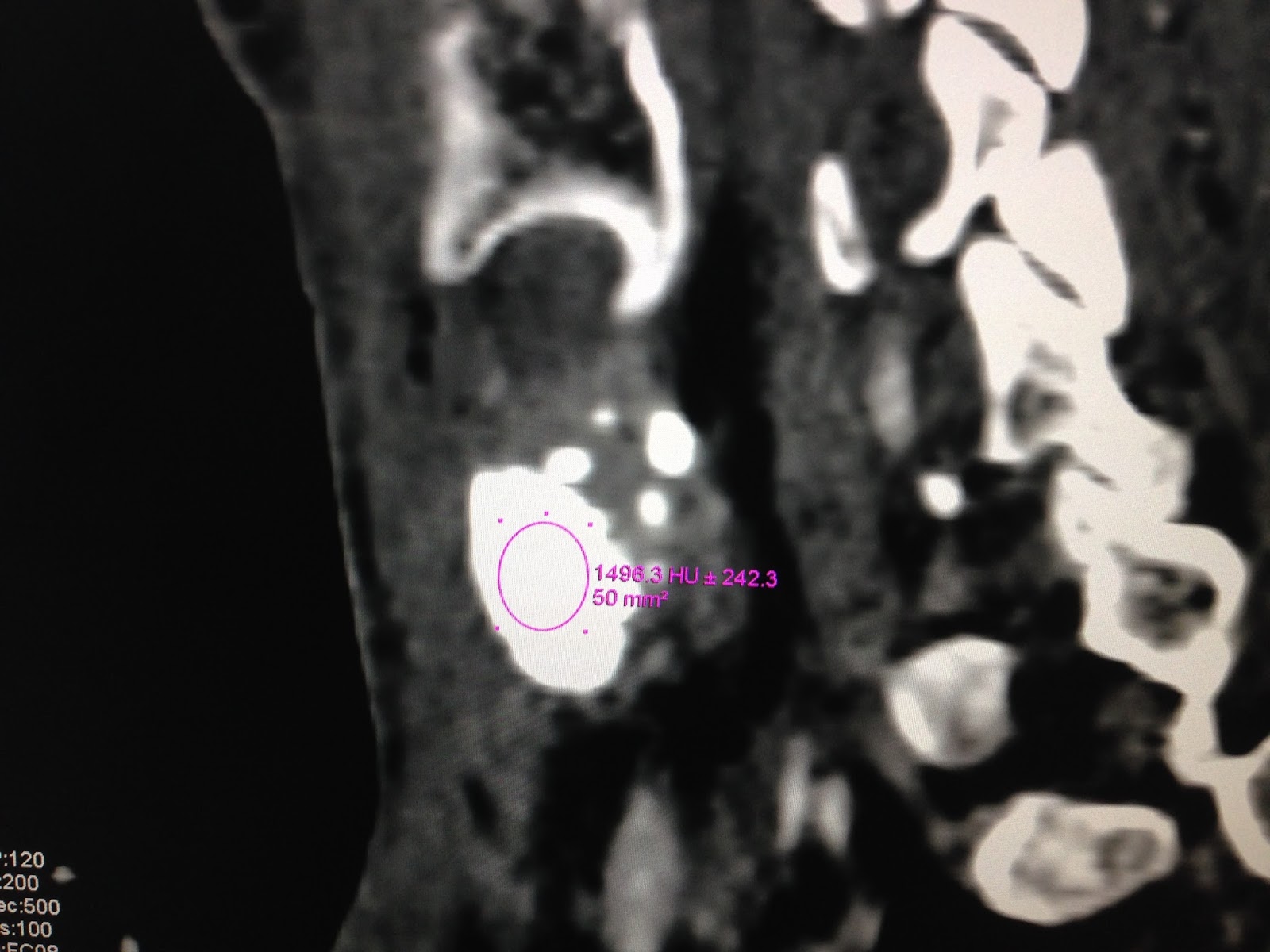
CT3 : frontal view with CE=HU of this mass is 1,319
UI

CT4: lymph node also has HU 1326UI.

CT5: sagittal view
this mass is covered near the righ lobe of thyroid gland.
Blood test TSH is 0,041 T4 1,2
TG 97,42 ( n 3, 5-77)
Pre-op diagnosis is thyroid cancer metastasis neck lymph nodes.
OPERATION REMOVED RIGHT THYROID GLAND AND LYMPHADENECTOMY.
SEE SPECEMEN
FOTO1 FOTO2 THYROID TUMOR CALCIFICATION


FOTO3 LYMPH NODE

CALCITONINE = 2PG/ML (M <18.2PG/ML)..RULES OUT MTC ( MEDULLARY THYROID CARCINOMA)
MICROSCOPIC REPORT OF SURGICAL SPECIMEN IS PAPILLARY CARCINOMA ( PTC) METASTASIS TO SOME LYMPH NODES.

SUMMARY = PTC WITH HUGE CALCIFICATION UNKNOWN.