Female patient 32 yo, loss of weight #10kg with epigastric pain and nausea for 2 months.


She herself took gastric drugs for a while but failed so went to Medic for a new examination.
Ultrasound of abdomen at Medic revealed many lymph nodes that were suspected metastatic nodes and mesenteric thickening; stomach walls infiltrated thickening and slight splenomegaly.



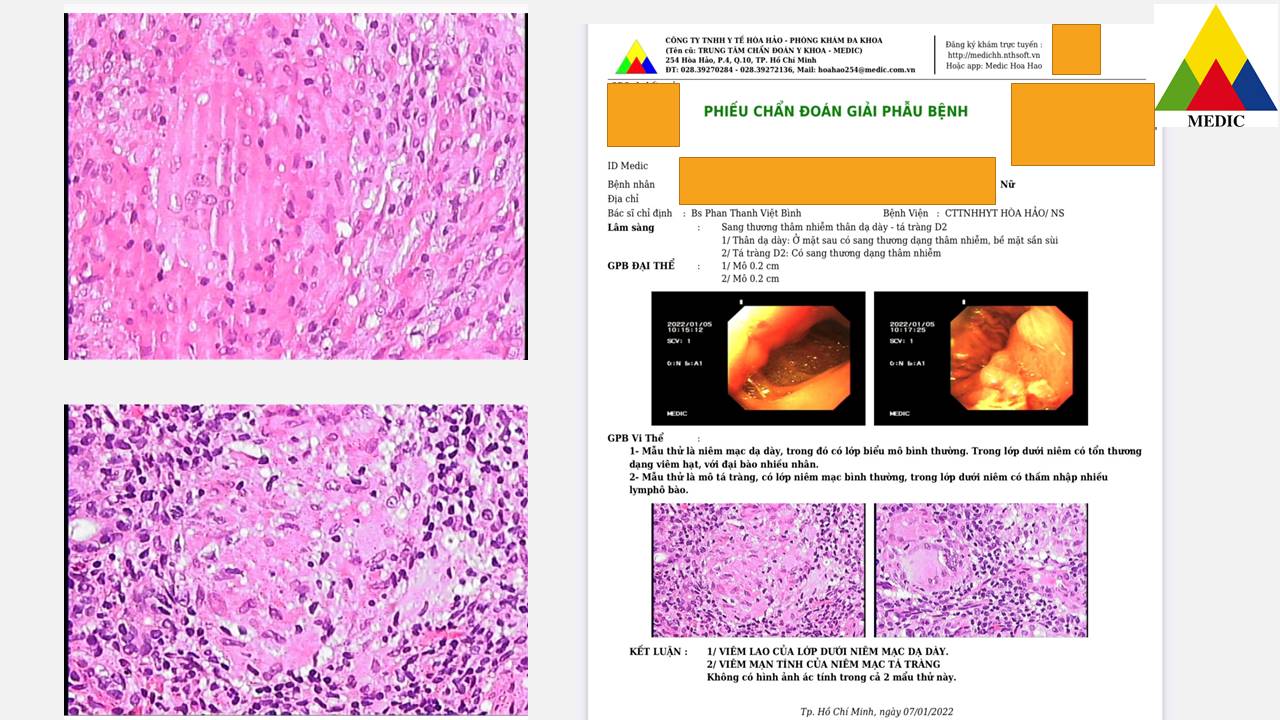
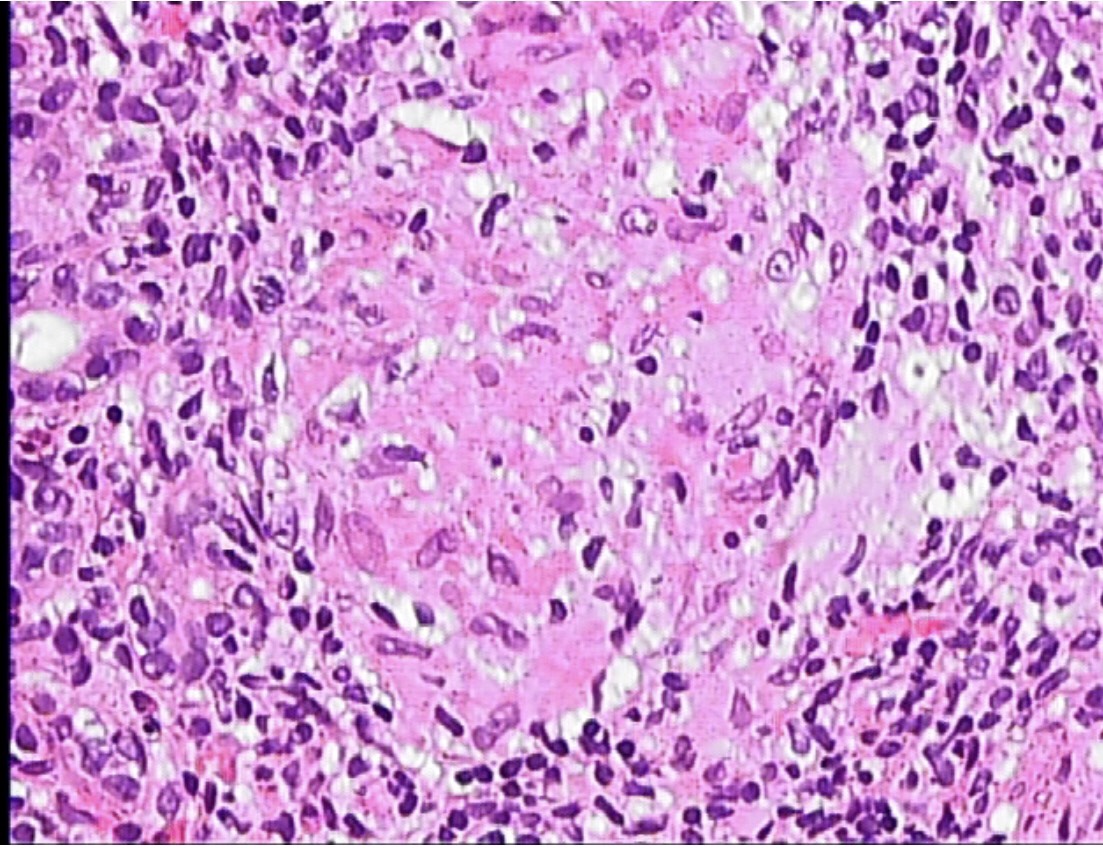
Gastric endoscopy showed gastric corpus roughly inflammed. Results of biopsy were inflammed submucosa layer of stomach and chronic inflammation of duodenum suspected due to TB infection.




MSCT confirmed that existed a lot of lymph nodes at hepatic hilus, lesser curvature of stomach, around celiac axis. These nodes maybe belong to TB nodes.



Result of biopsy of intraabdominal lymph nodes was TB inflammed nodes.



Discussions and Conclusions
TB of stomach is still a rare entity, which is about 1-2% of GI tract tuberculosis and in 0.5% of patients contracted with TB. Usually it is secondary after the pulmonary TB infection.
Our patient is now getting better status, gained more 2 kg of weight while being taken TB drugs for 2 months of 6 month-regimen of therapy.