Male patient 83 yo with unknown cause of fever (T. 38-39 degree of Celsius) for one week. And nothing abnormal detected in clinical examination.
A full body MSCT detected a big #90x60 mm gallbladder [GB] which existed a bile debris-fluid level and #6mm thickened GB wall. Edema around GB bed was noted. A diagnosis of acute cholecystitis was done but without cause.


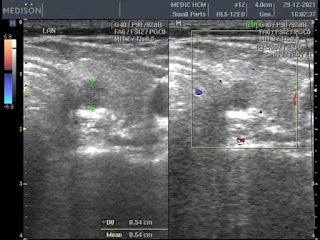
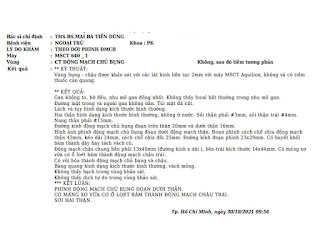
Later, ultrasound looks for cause of big GB status that shows bile debris of 12 mm into # 7 mm dilated GB duct and GB wall edema #16 mm. No fluid is seen around the GB. Beside GB, it exists an hepatic area of GB bed #53x28 mm which has been edema, not well limited, seems to be infiltrated and no mass effect. Also there are some Rokitanski sinii # 35 mm in GB wall. CBD and intrahepatic bile ducts are re not dilated and without stone. An obstruction of neck of GB that causes hydrops of GB and leads to complication of acute cholecystitis with inflammation of GB bed area.




Lab data CRP 157, WBC 10.14 [neutro 75%].
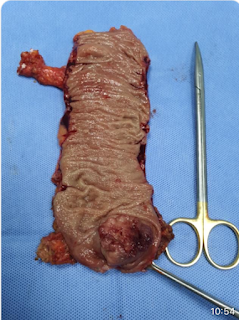
PIV antibiotics for acute cholecystitis in one week and later, laparoscopic cholecystectomy was done to remove the big gallbladder.

Macroscopic specimen of pyo cholecystitis without stone
Microscopic result is chronic cholecystitis.

Reference