Woman 45 yo with fever and
cough. Chest XRays detected many white spots like balloon both site
the lung.
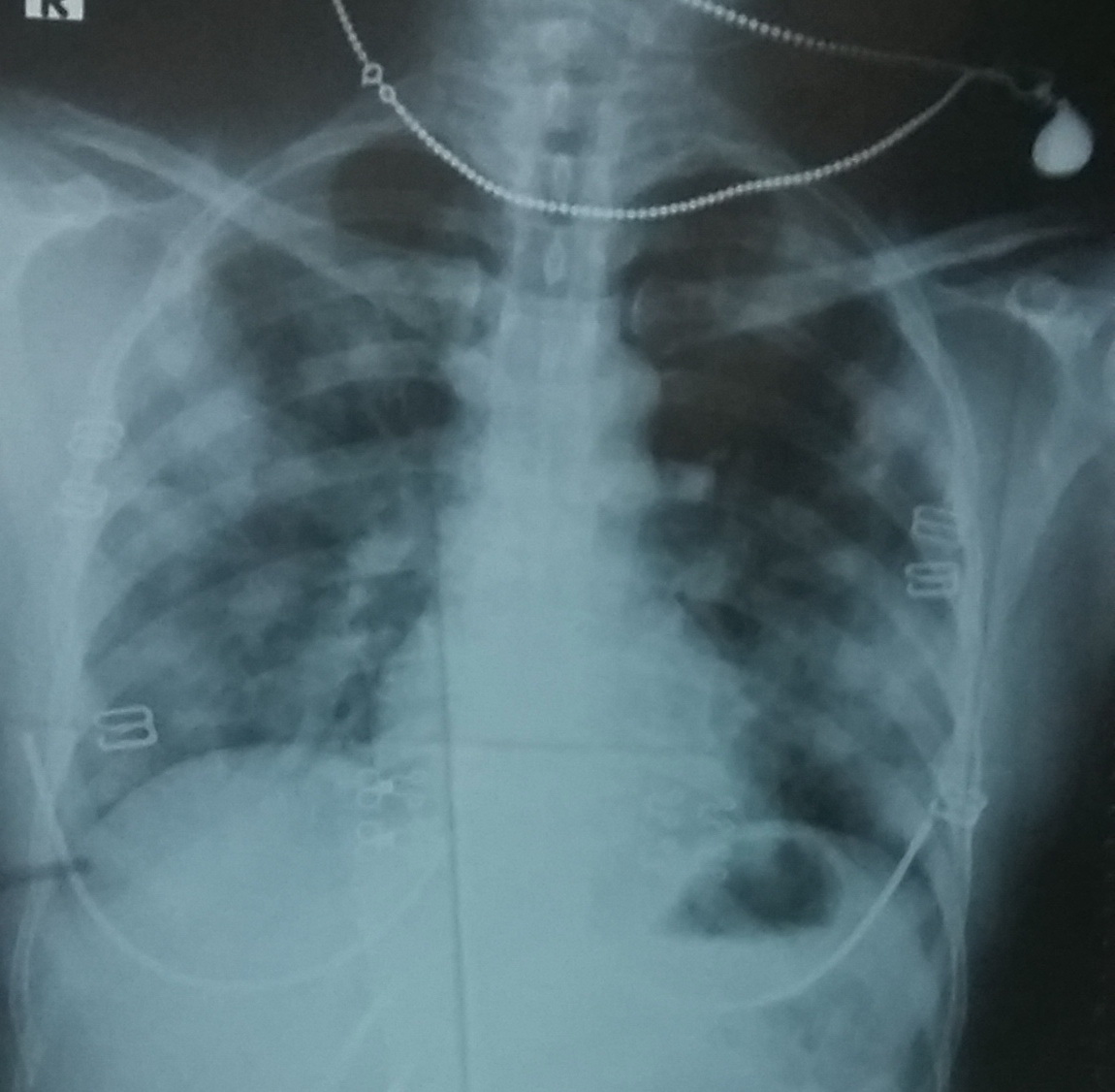
Radiologist suggested diffuse lung metastasis.
Blood tests= WBC rise 11.27 k, eosi
20,7%, IgE 1779 UI/mL.
Toxocara sp positive with od
1,809 and all cancer marker are negative.
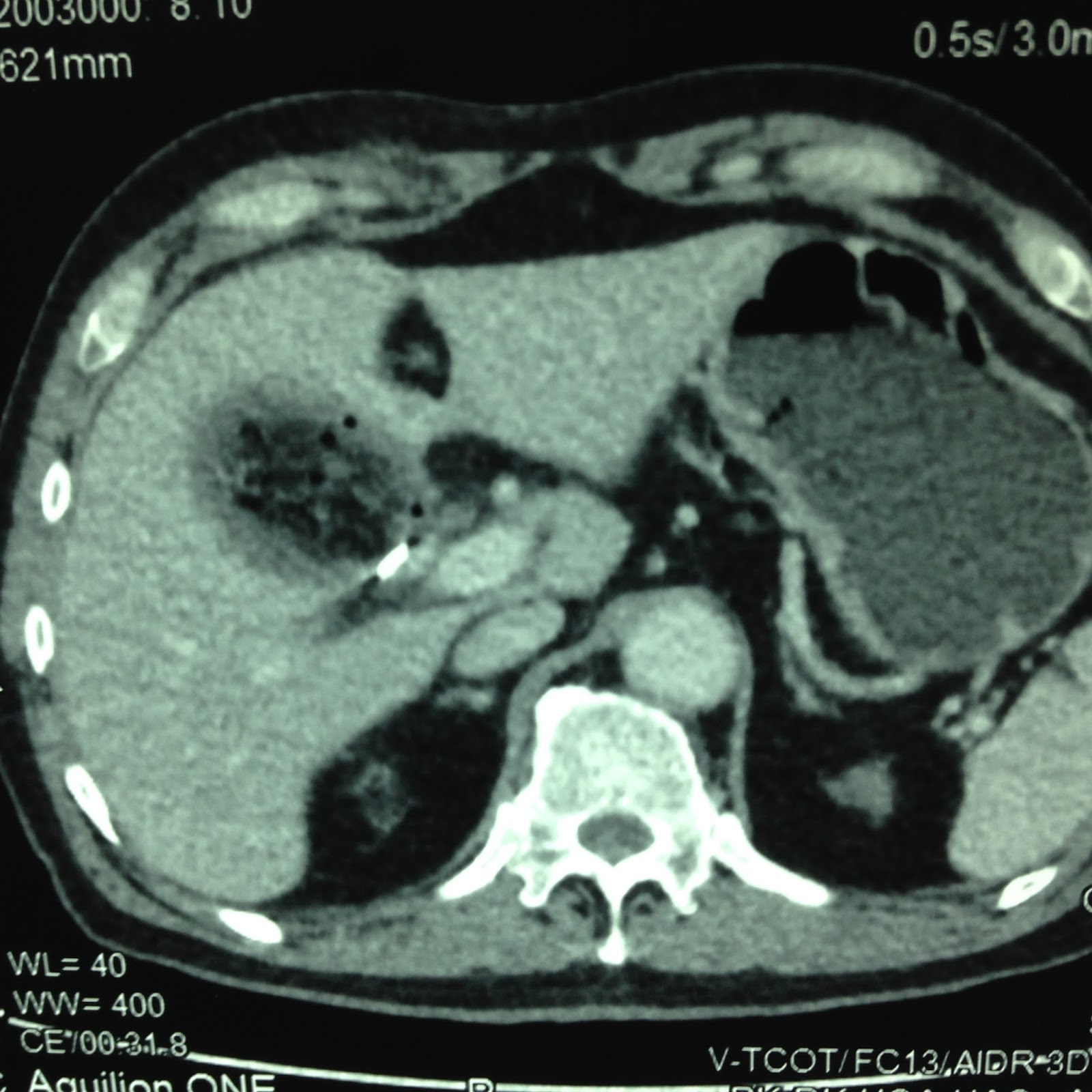
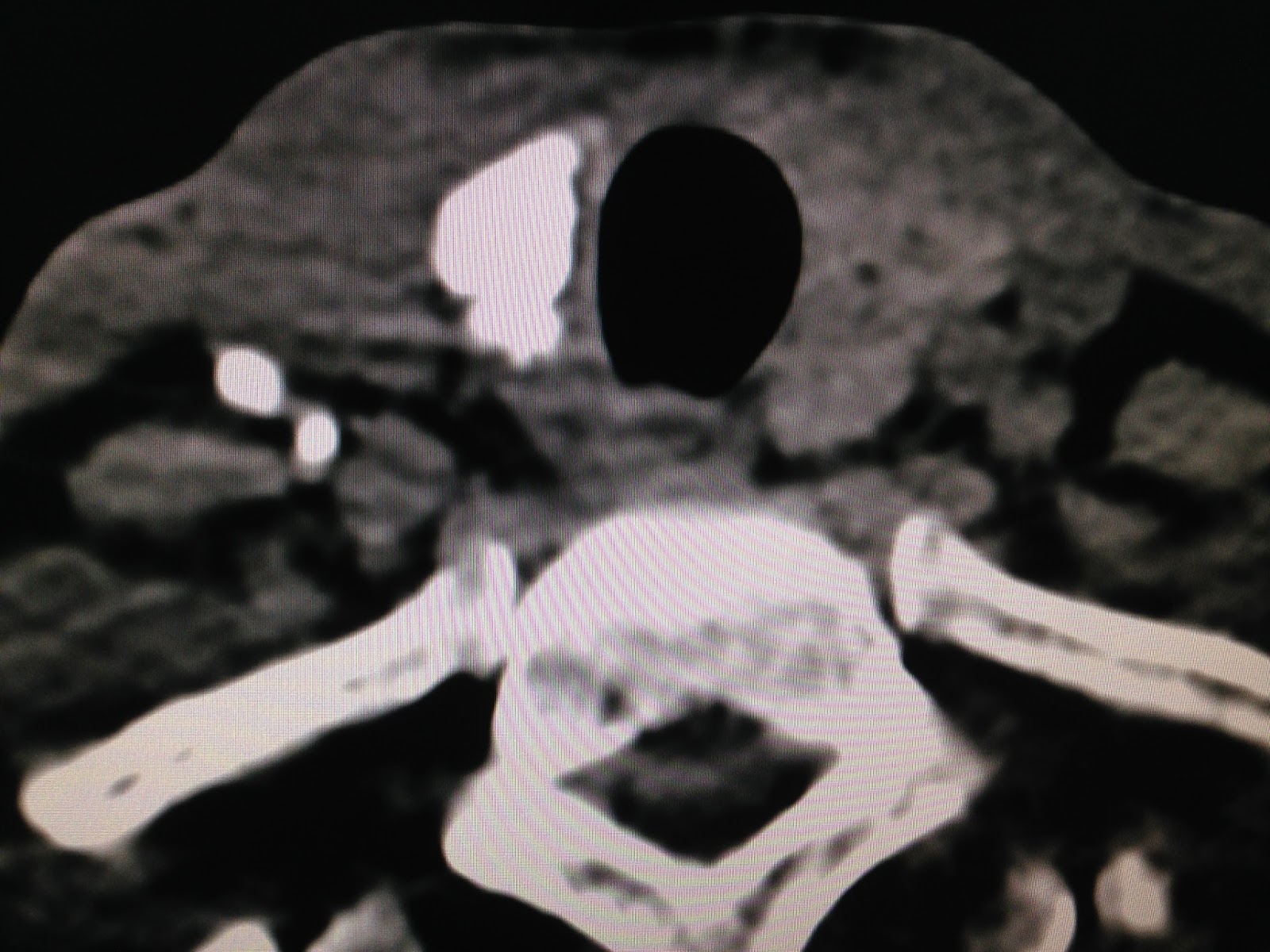
CT scan with CE many opacification of
peripheral lung booth site( CT1a/b)


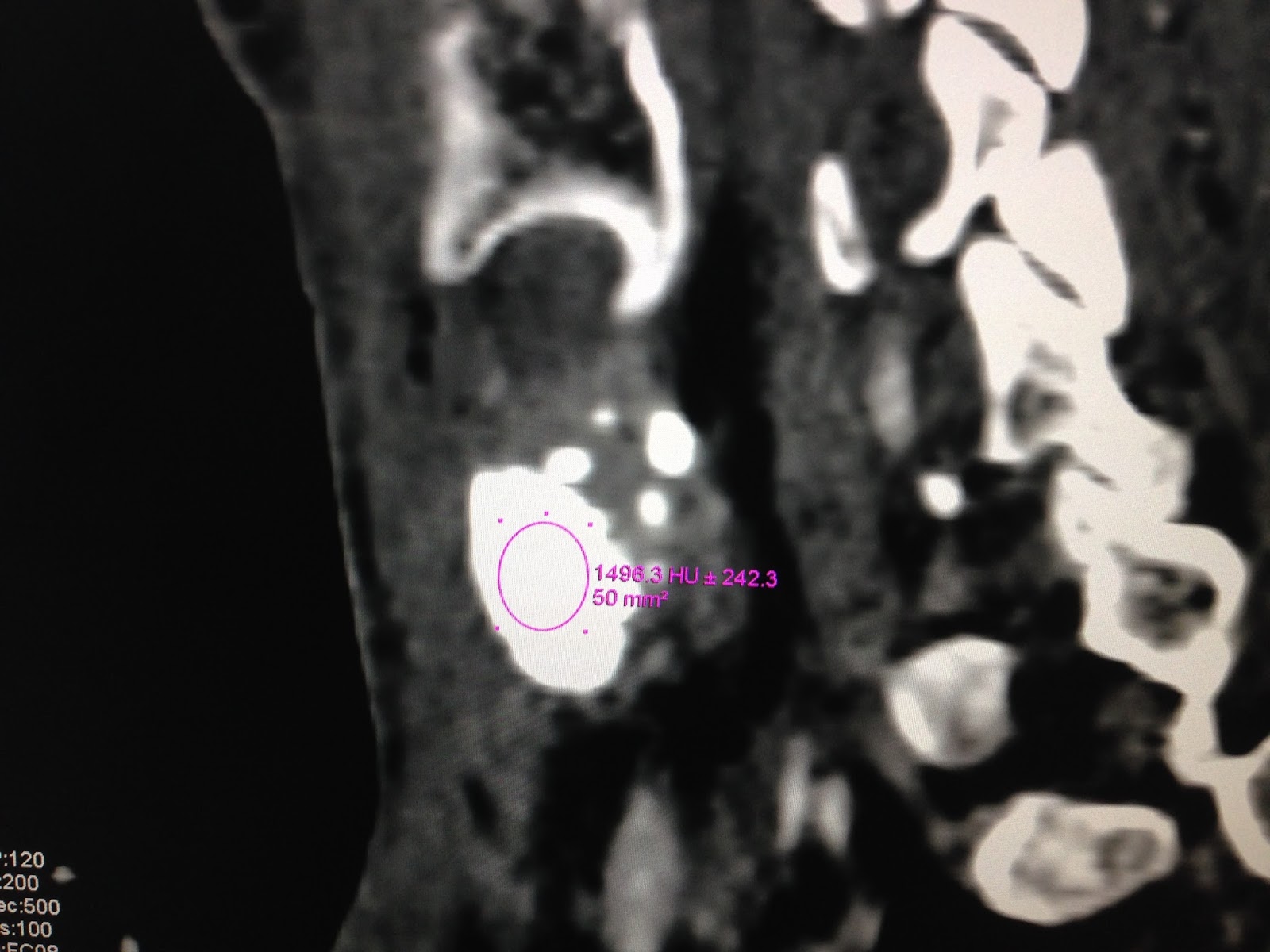
CT scan the lung with CE the
lesion is small regression.

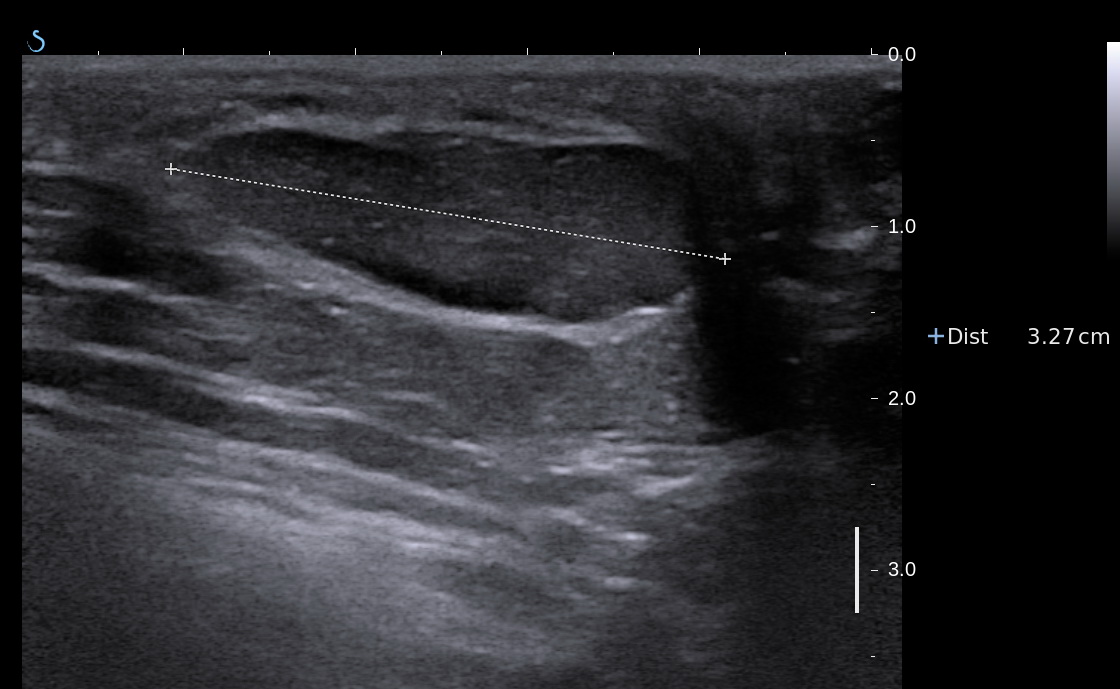
Ultrasound of thorax with small light

After one week treatment no fever
no cough. Chest Xrays is clear.

Summary: By the clinical, blood
tests, chest XRays, diagnosis
as Loffler syndrome of the lung was made for the case.
REFERENCE


REFERENCE