Woman
35 yo detected at right axiilary a soft and
bigger mass. Clinical looked like a lipoma.
Ultrasound scan of this mass :
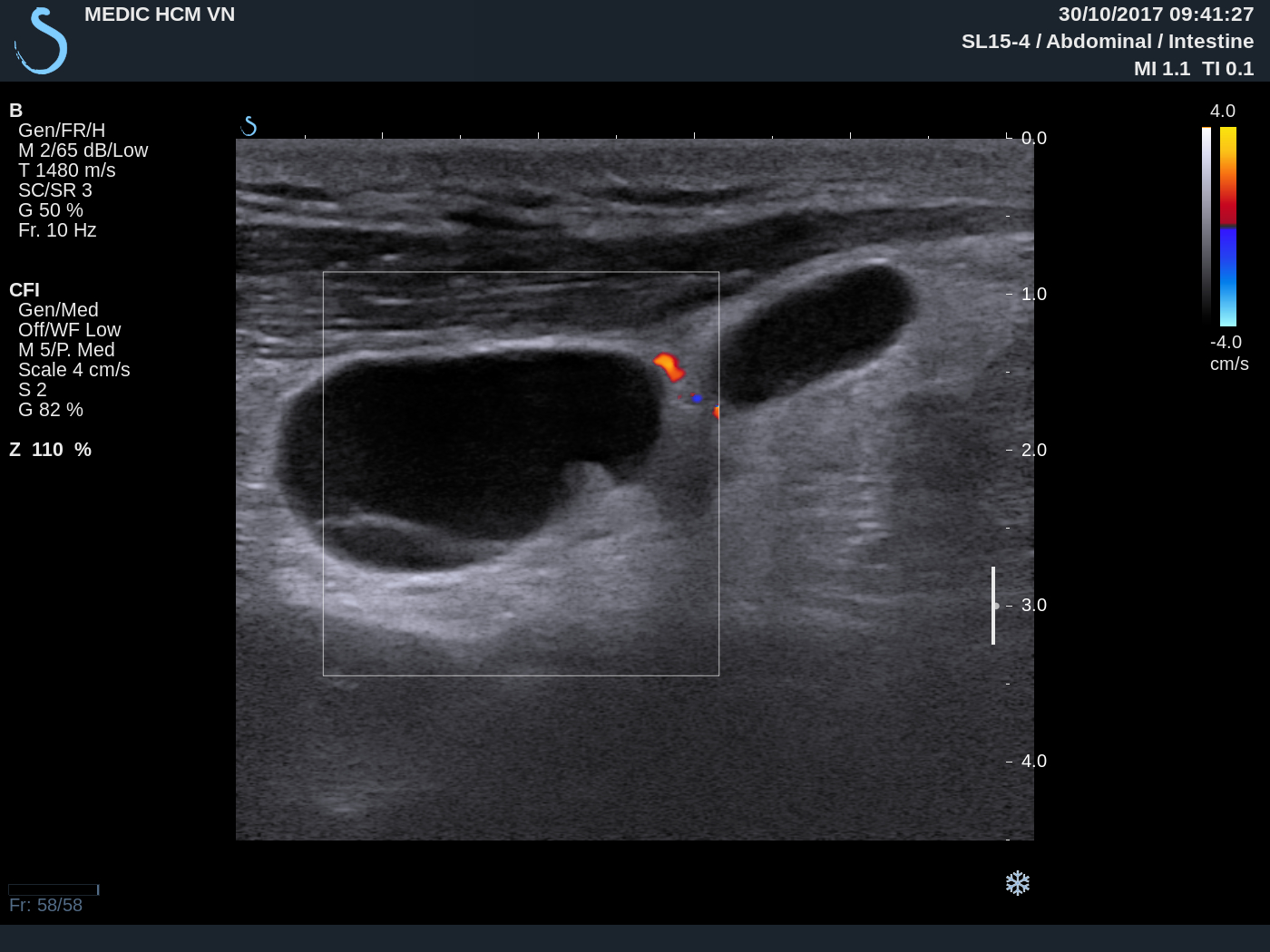
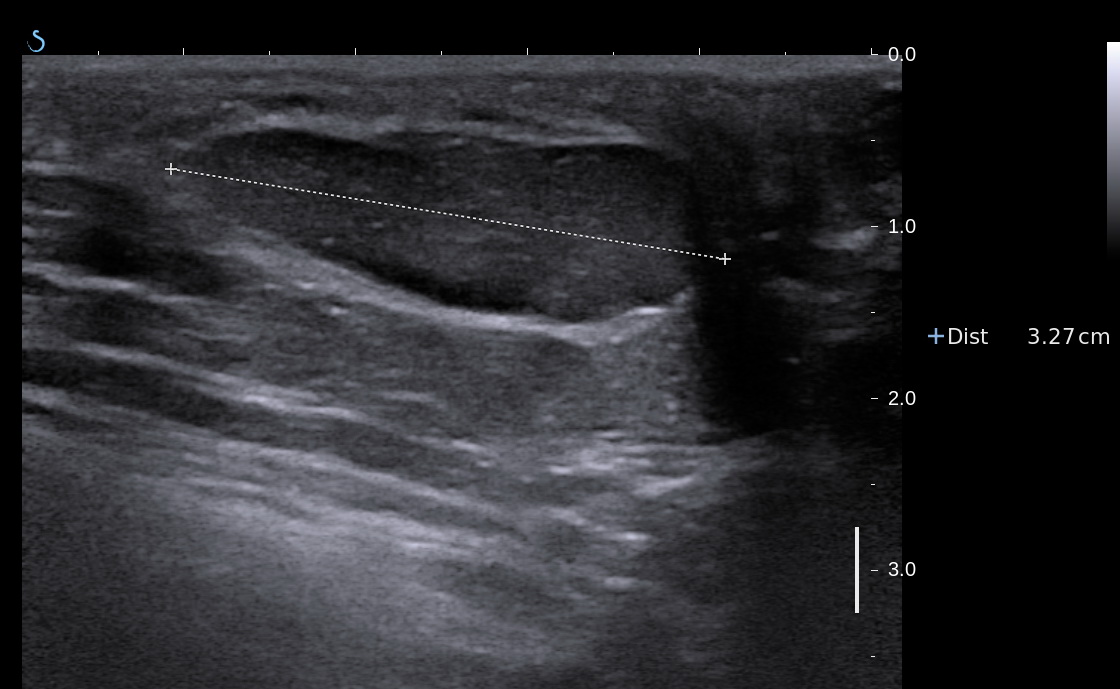
US 1:
longitudinal scan= subcutaneous hypoechoic
mass, size 4cm, well bordered.
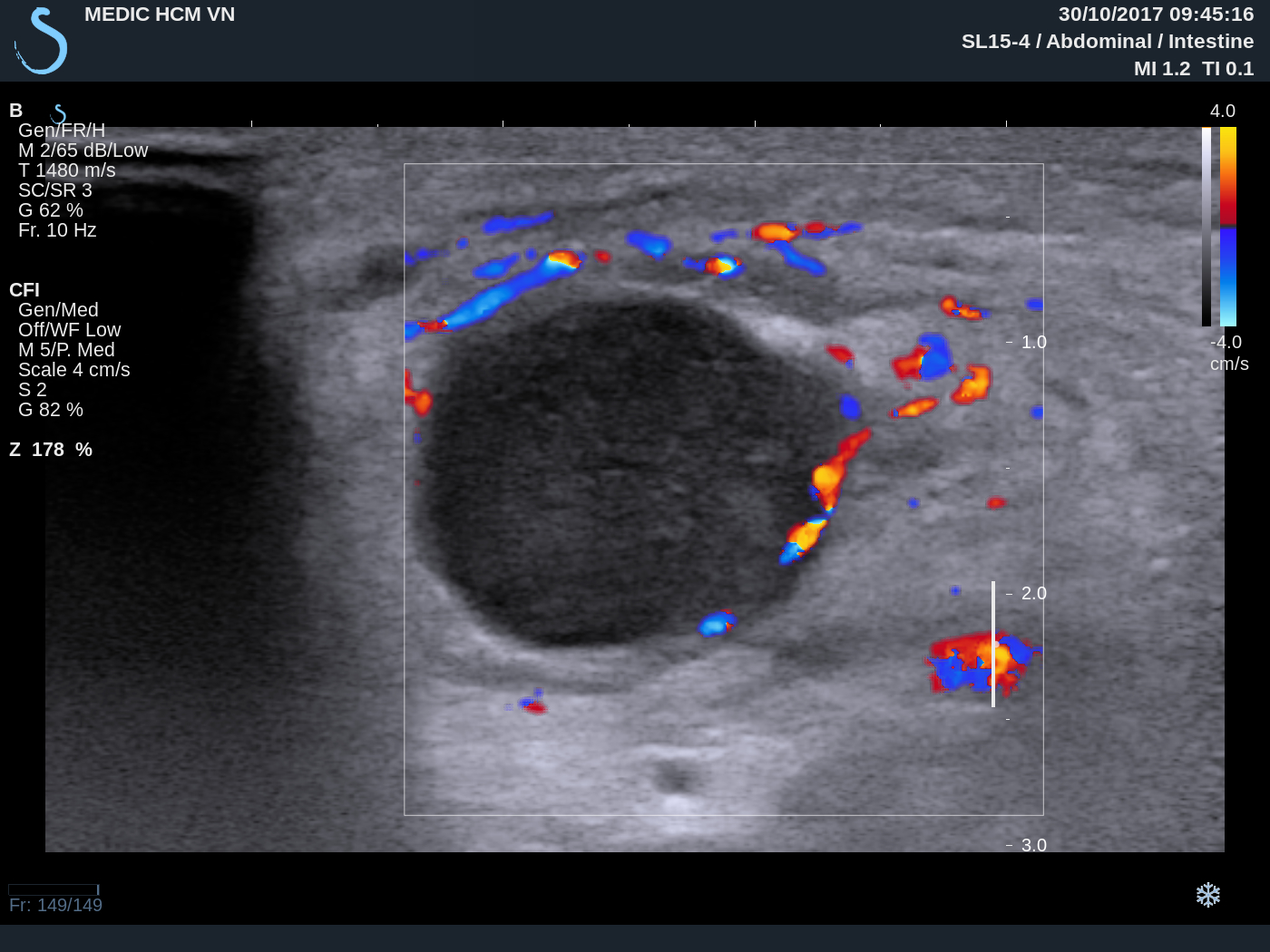
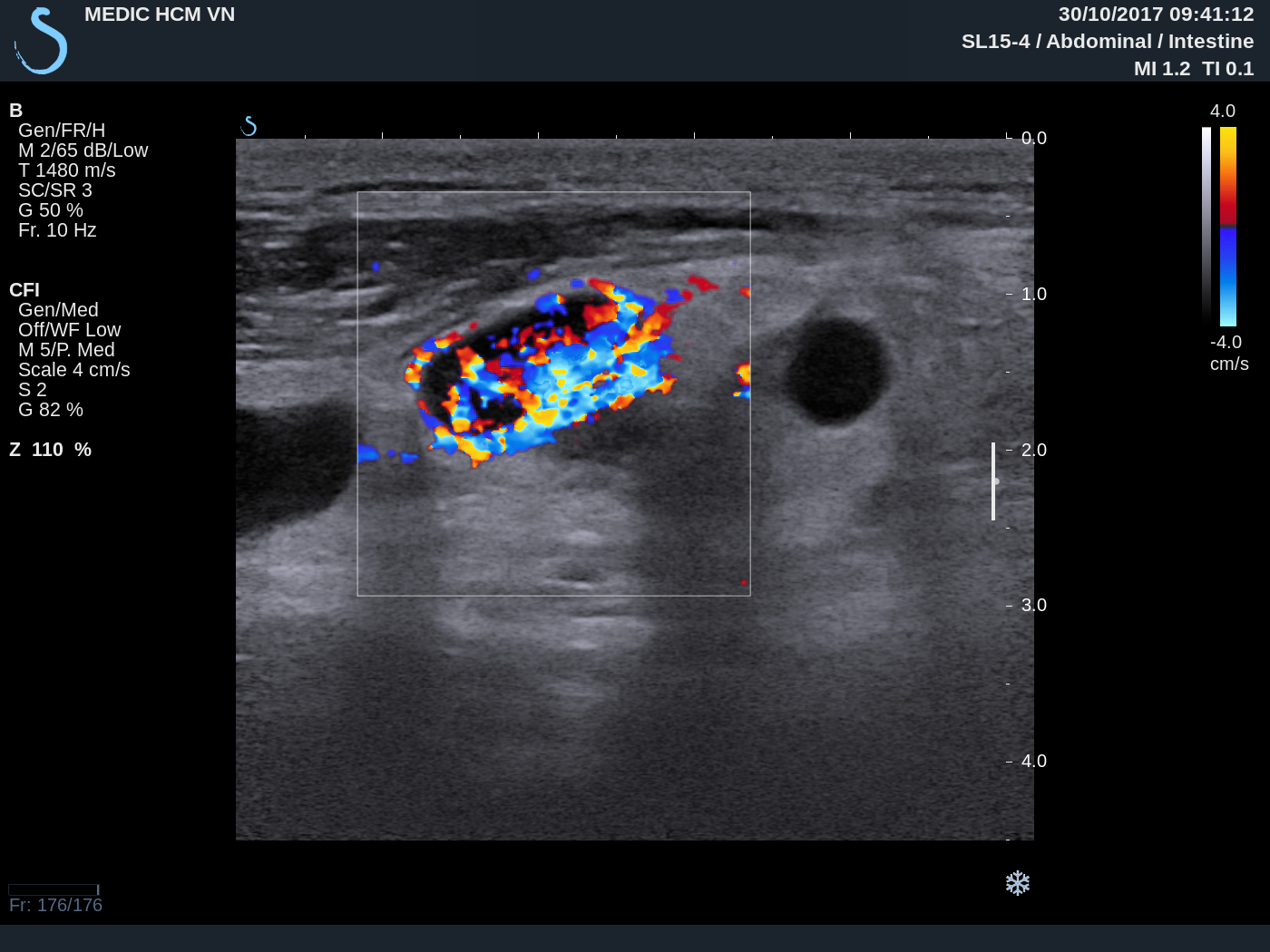
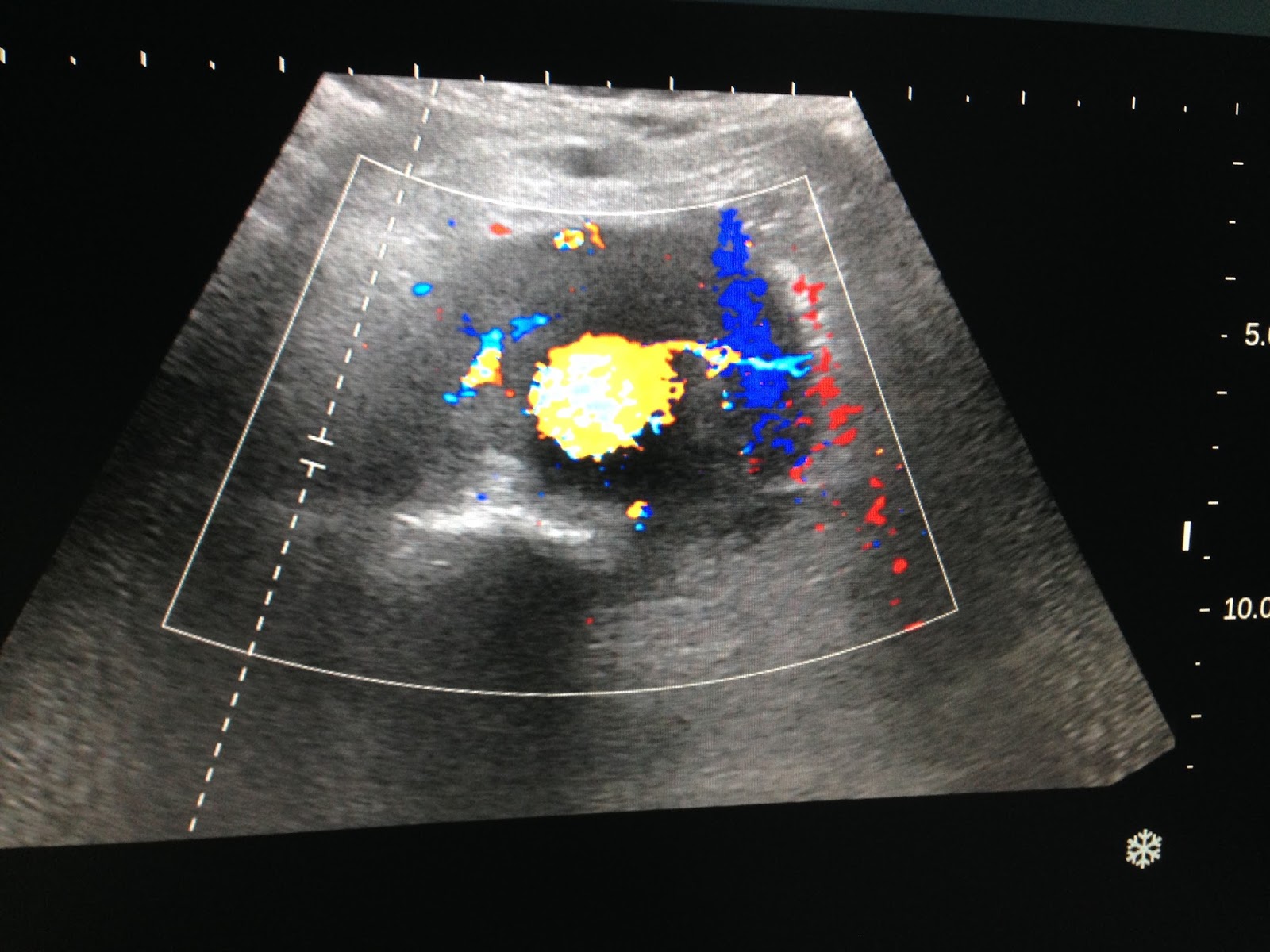
US 2: CDI
hypovascular pattern.

US 3:
elastoscan of this mass = 4.3 kPa, like fatty
tissue.

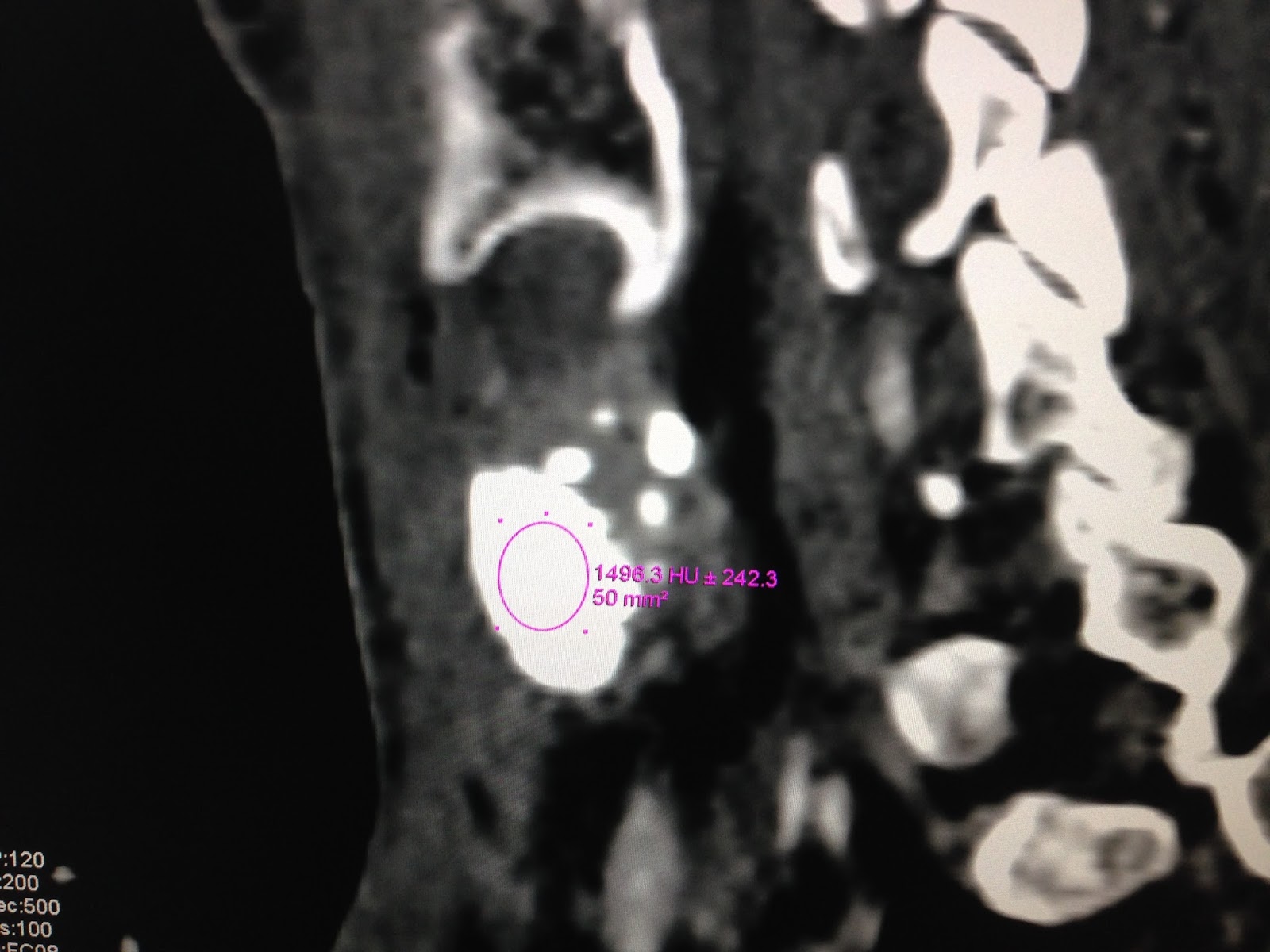
MSCT
non CE:
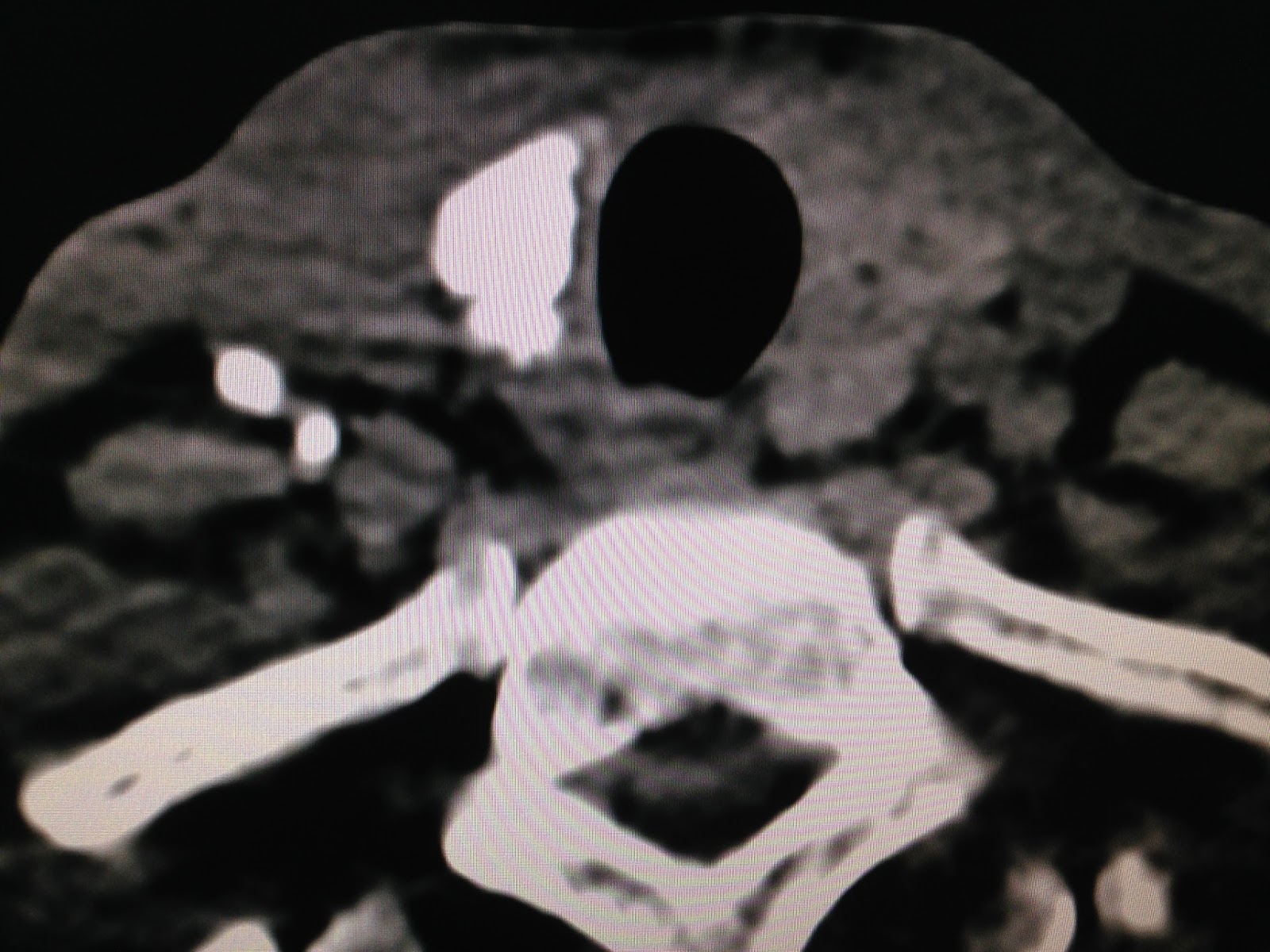
CT 1:
frontal view of this mass =
subcutaneous, same density of fatty tissue.

CT 2 : zooming of this mass showed structure looked like a nipple of breast.

CT 3:
crossed-sectional view of this
mass = well bodered, not connected to the right breast.

CT 4: sagittal
view of this mass= separation to the right breast.

Radiologist
reported an axillary mammary gland.
Operation
for removing this mass
(see foto specimen),

surgeon reported it having fatty and hard tissue. Microscopic report is tissue of mammary gland.

Summary of this
case: axiilary mammary gland mimicking as a lipoma mass.