Man 43 yo with epigastric
pain crisis and gastroendoscopy showed
gastritis.
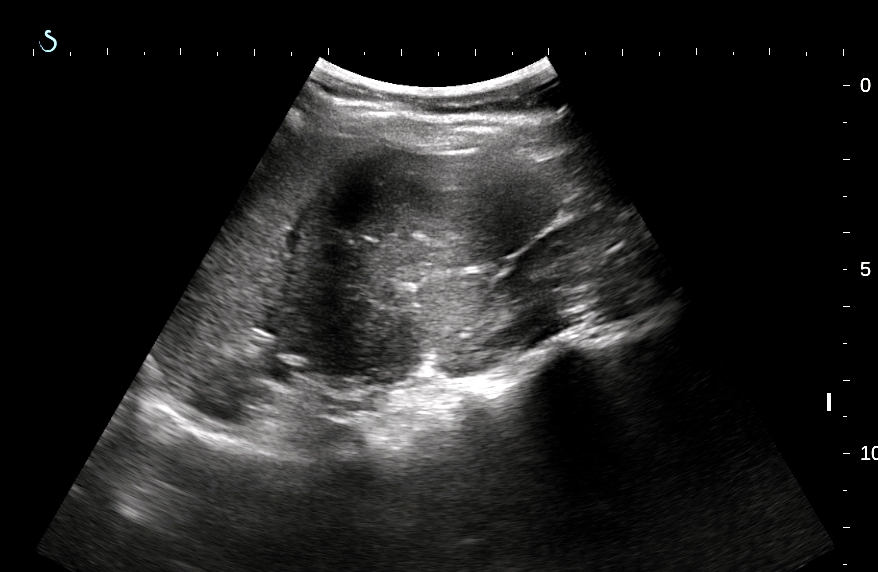
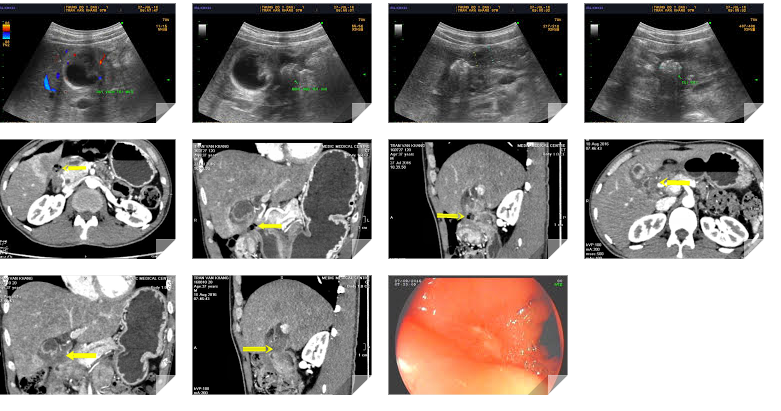
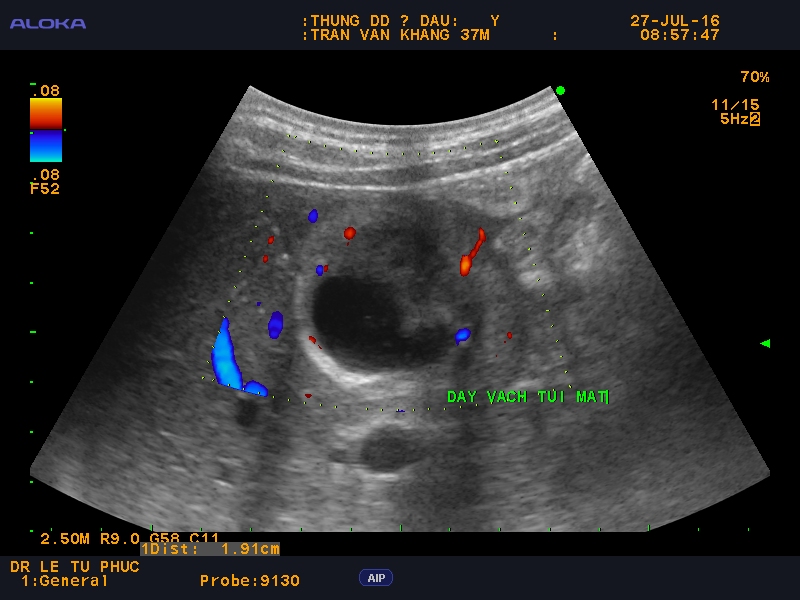
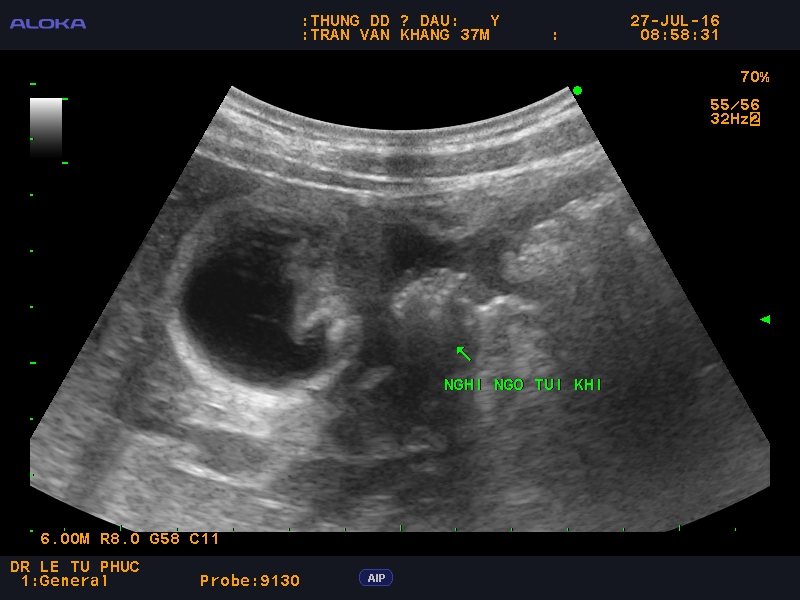
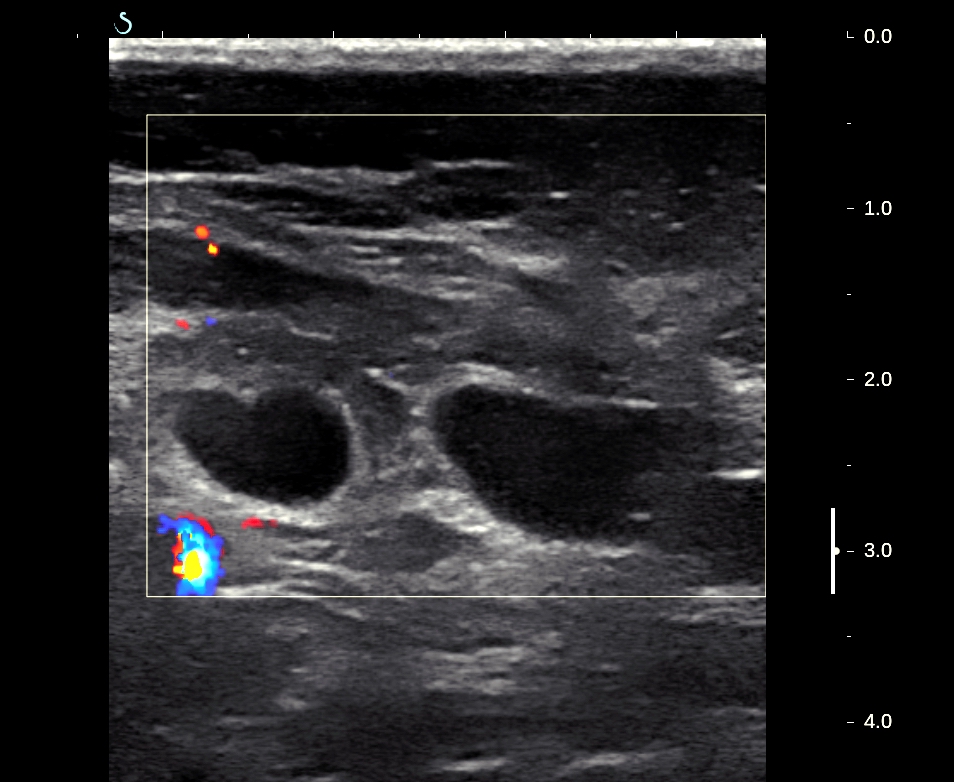
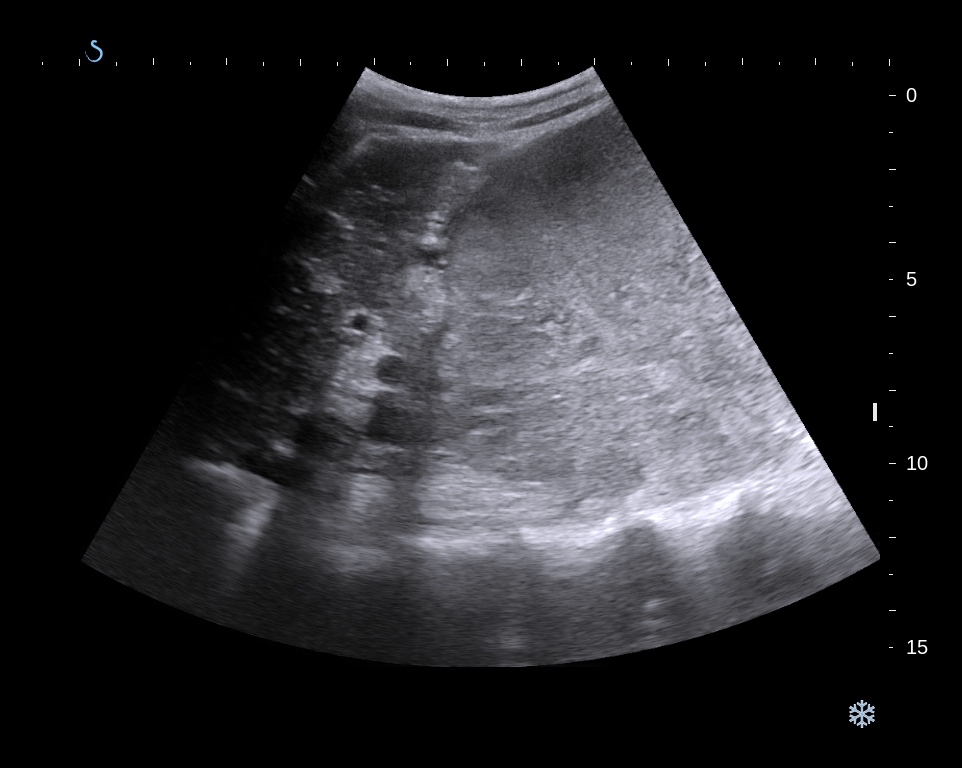
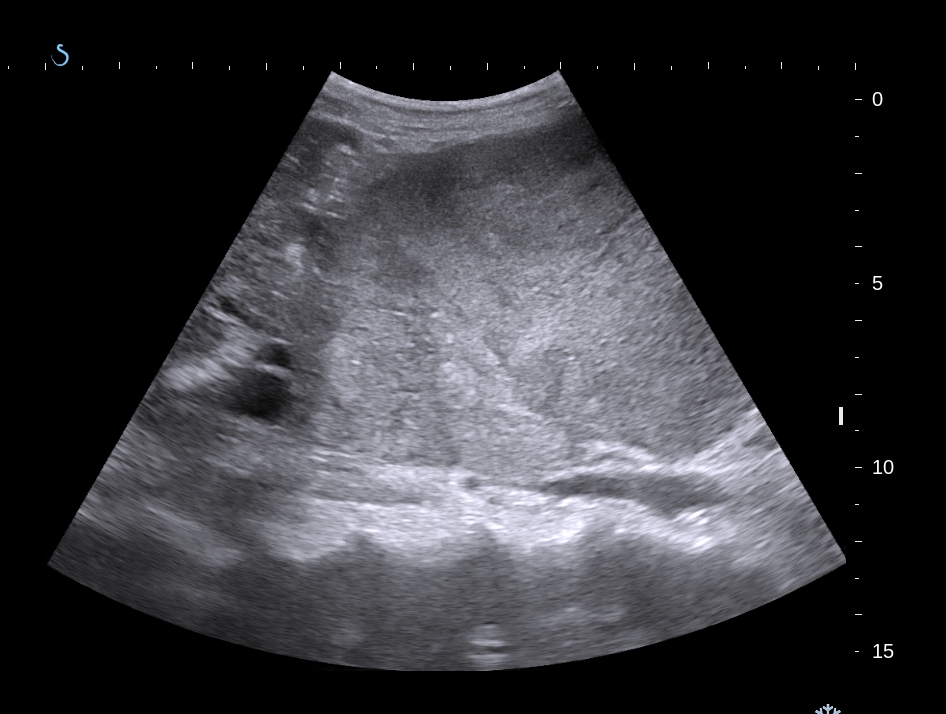
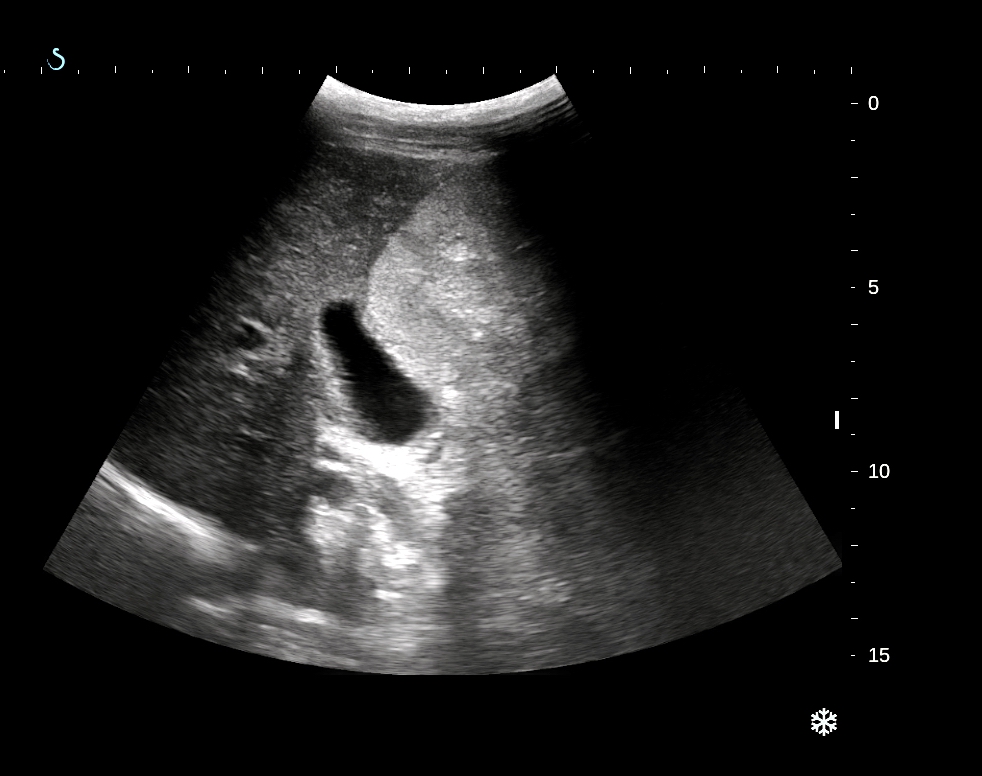
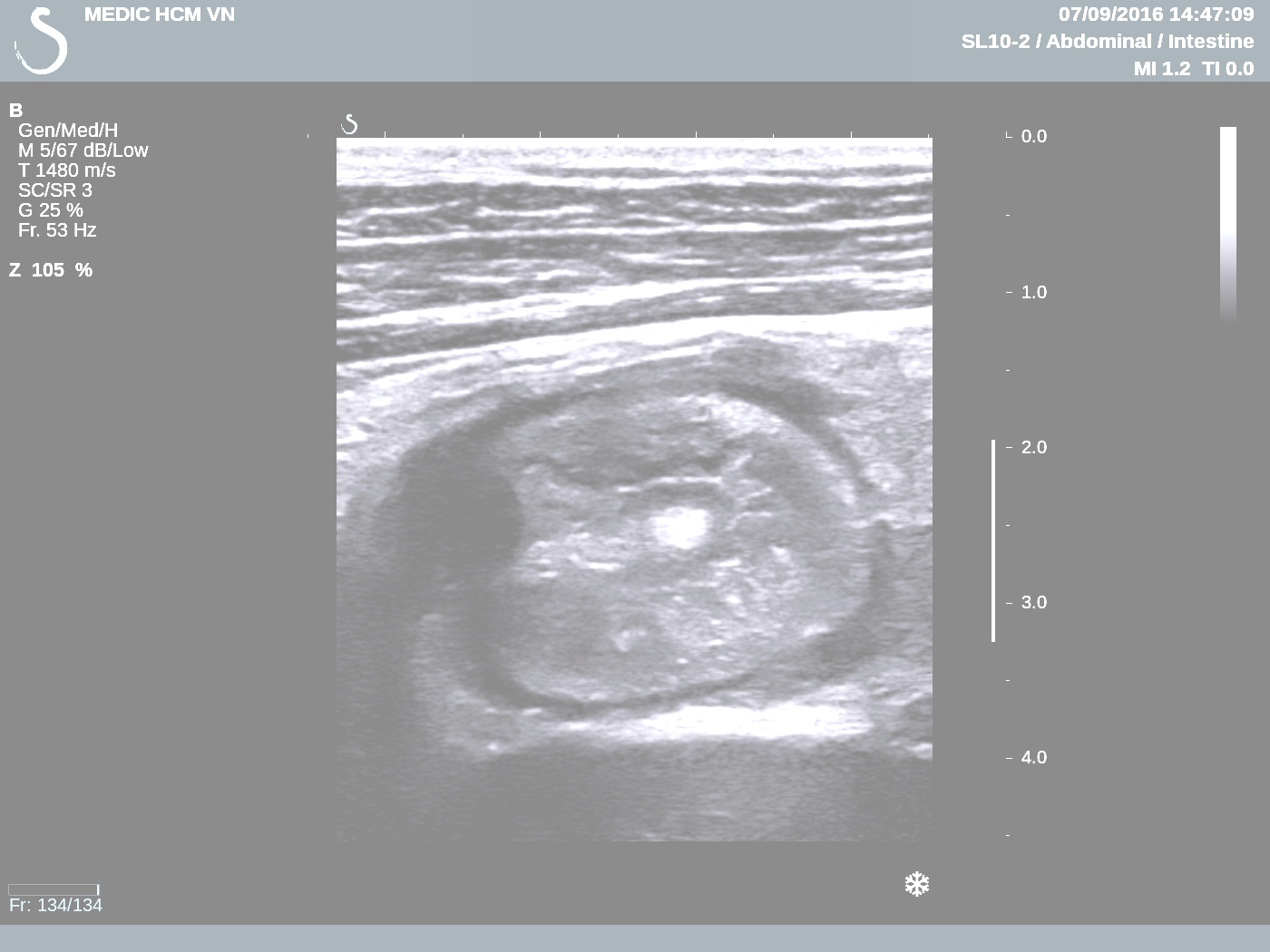
Ultrasound detected
one mass like target with
thickening of the wall of colon (see US 1=csoss-section
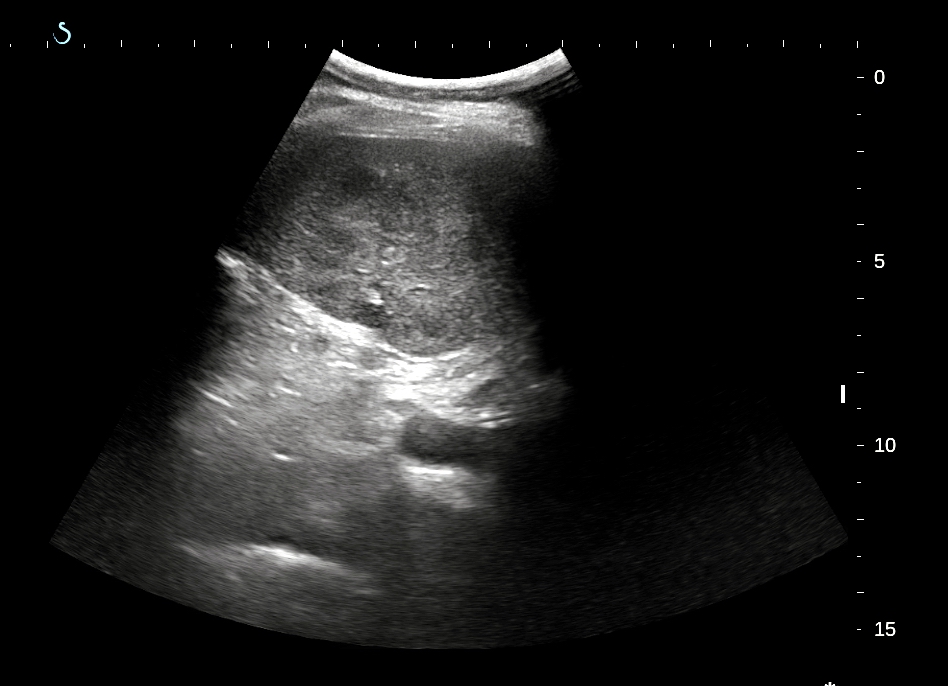
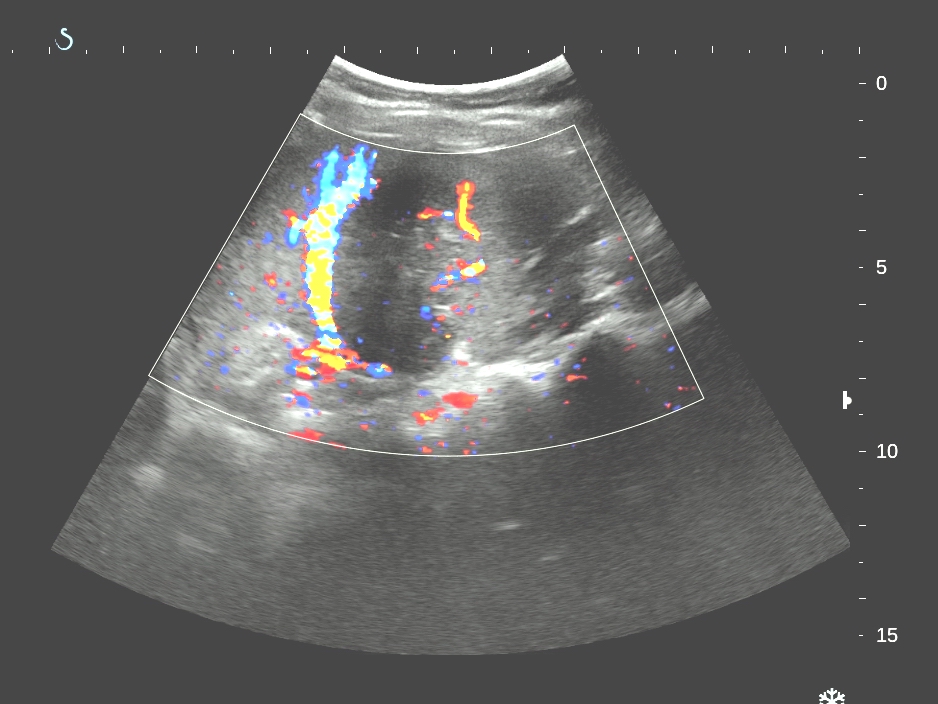
colon over right kidney); US
2 with linear probe= colon
wall is thickening; US 3, US 4 = longitudinal scan).



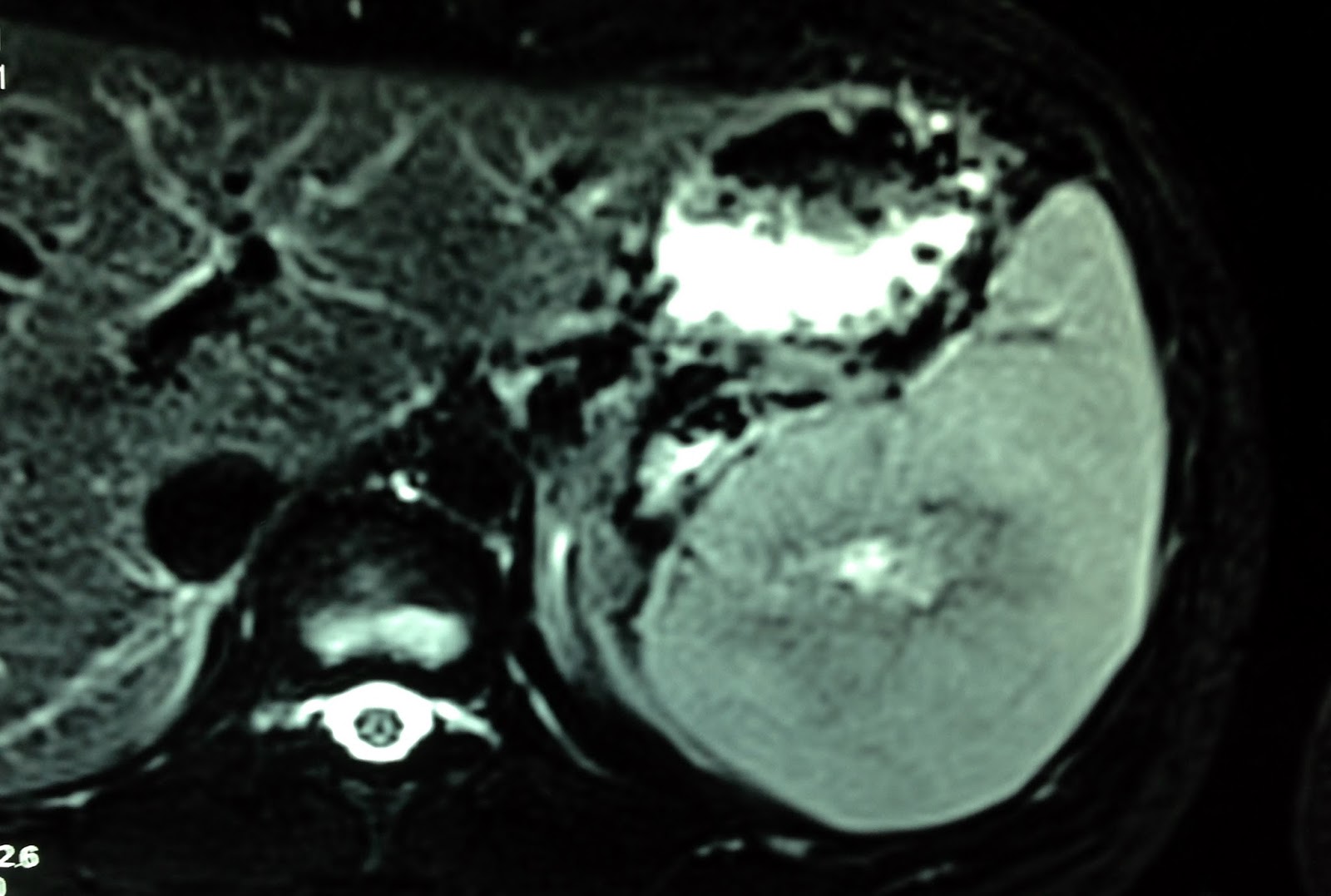
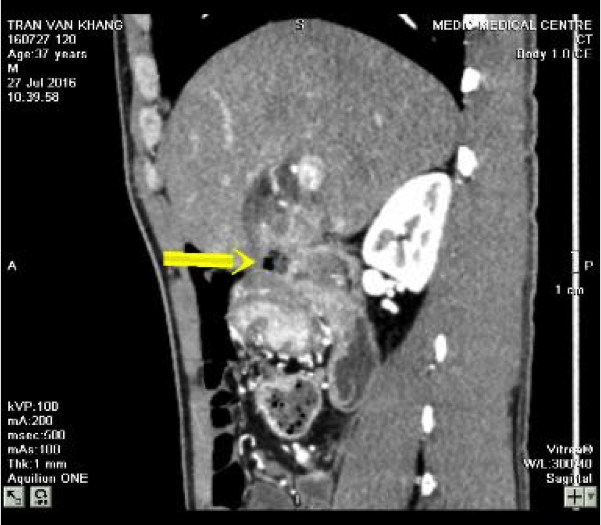
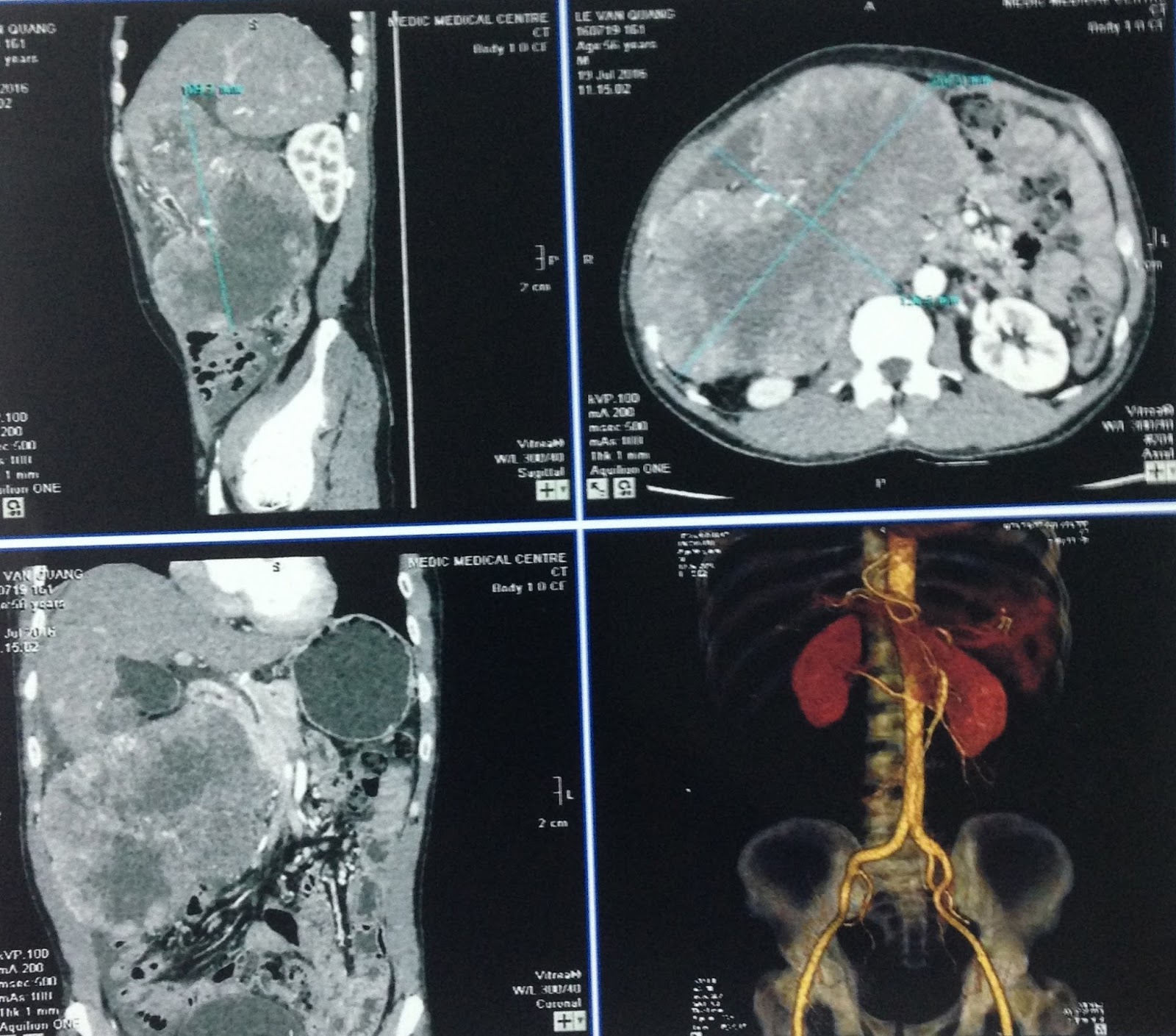
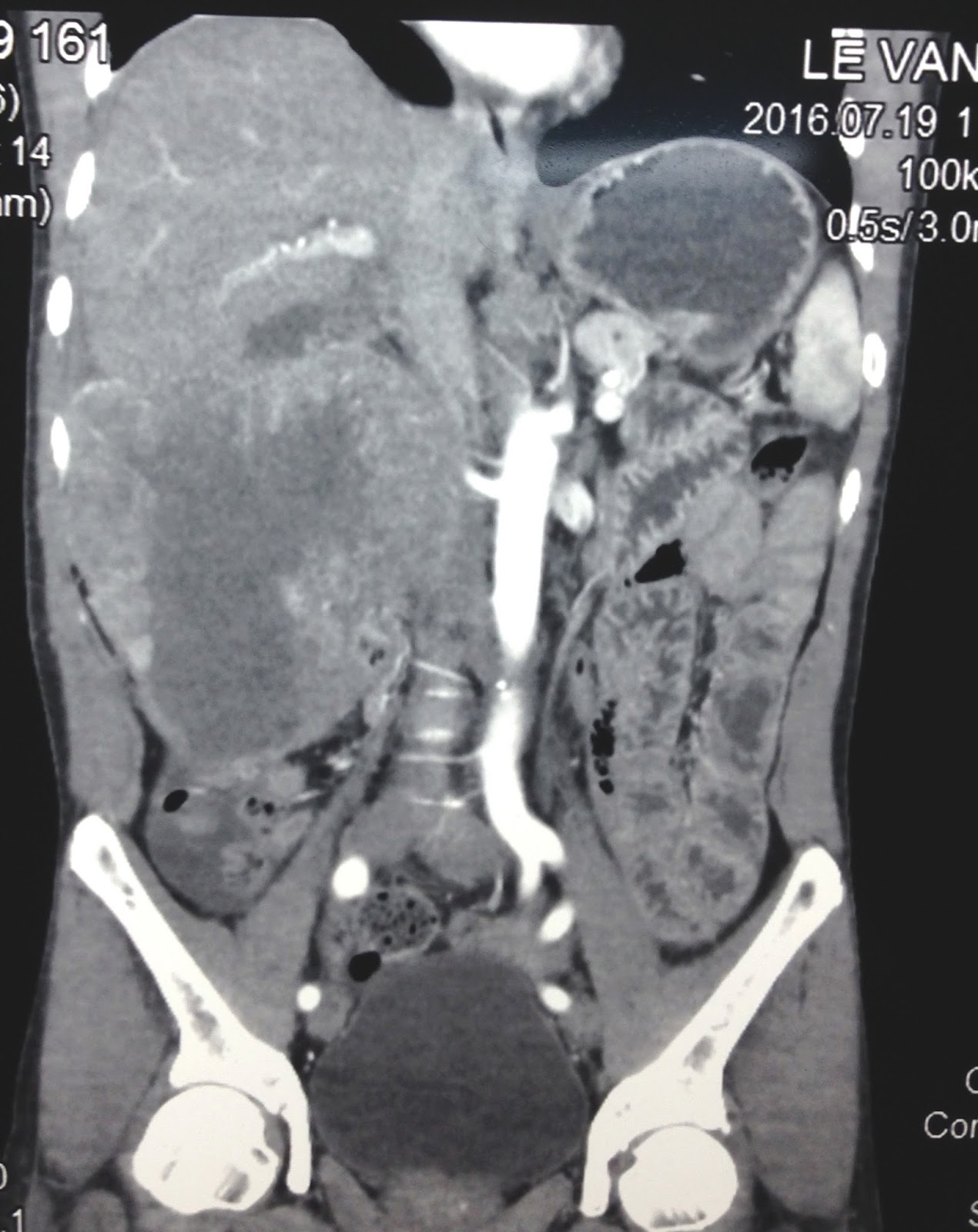
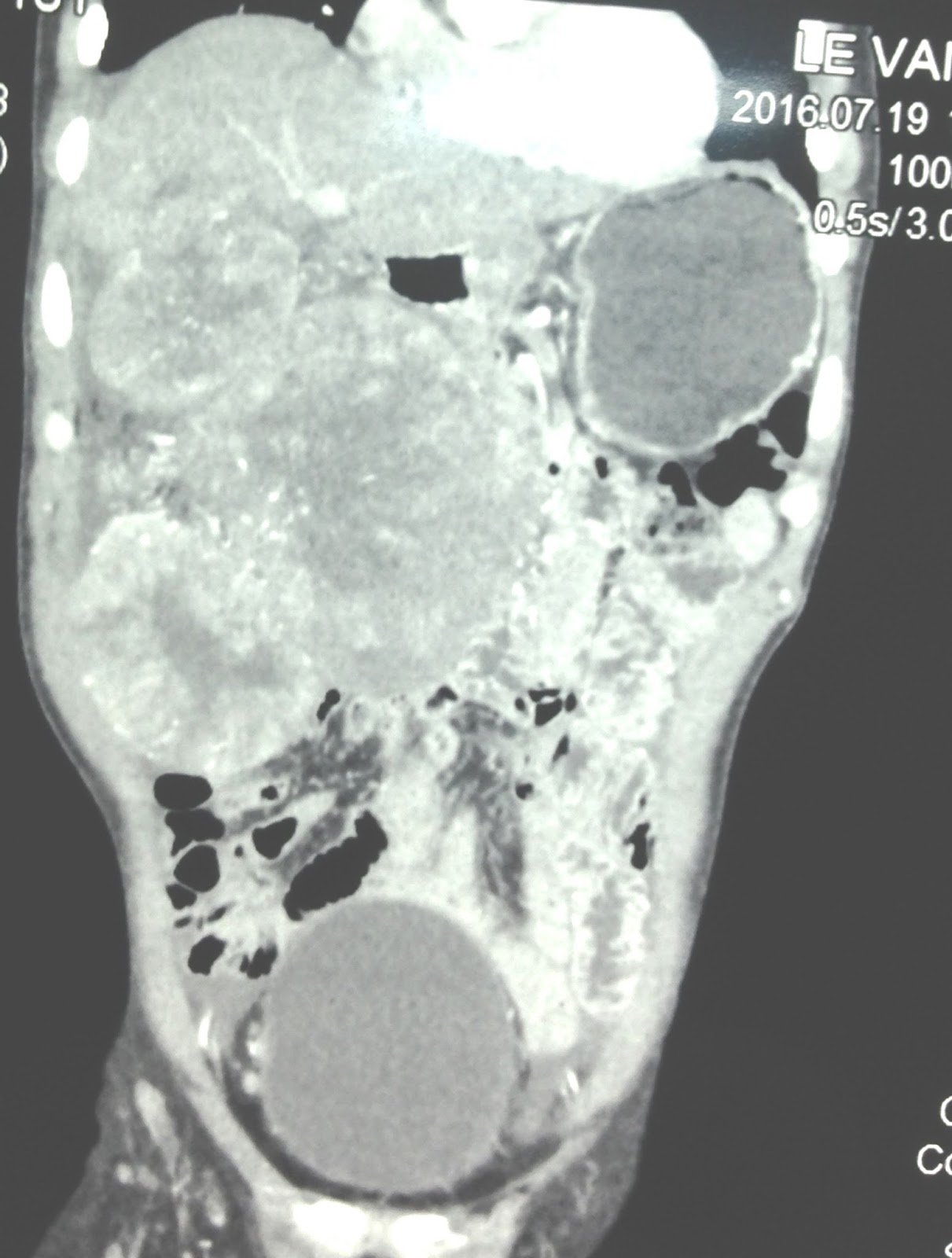
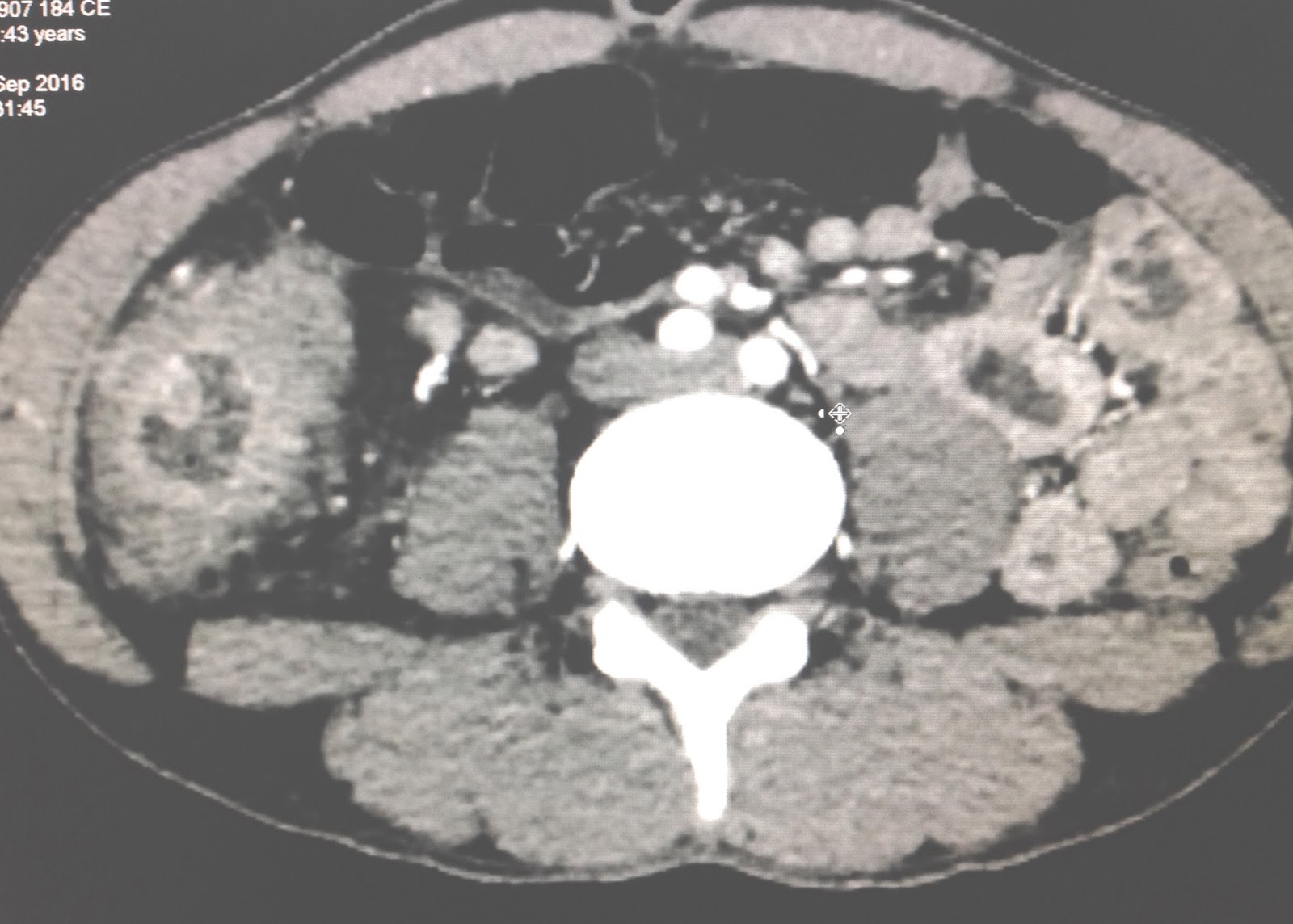
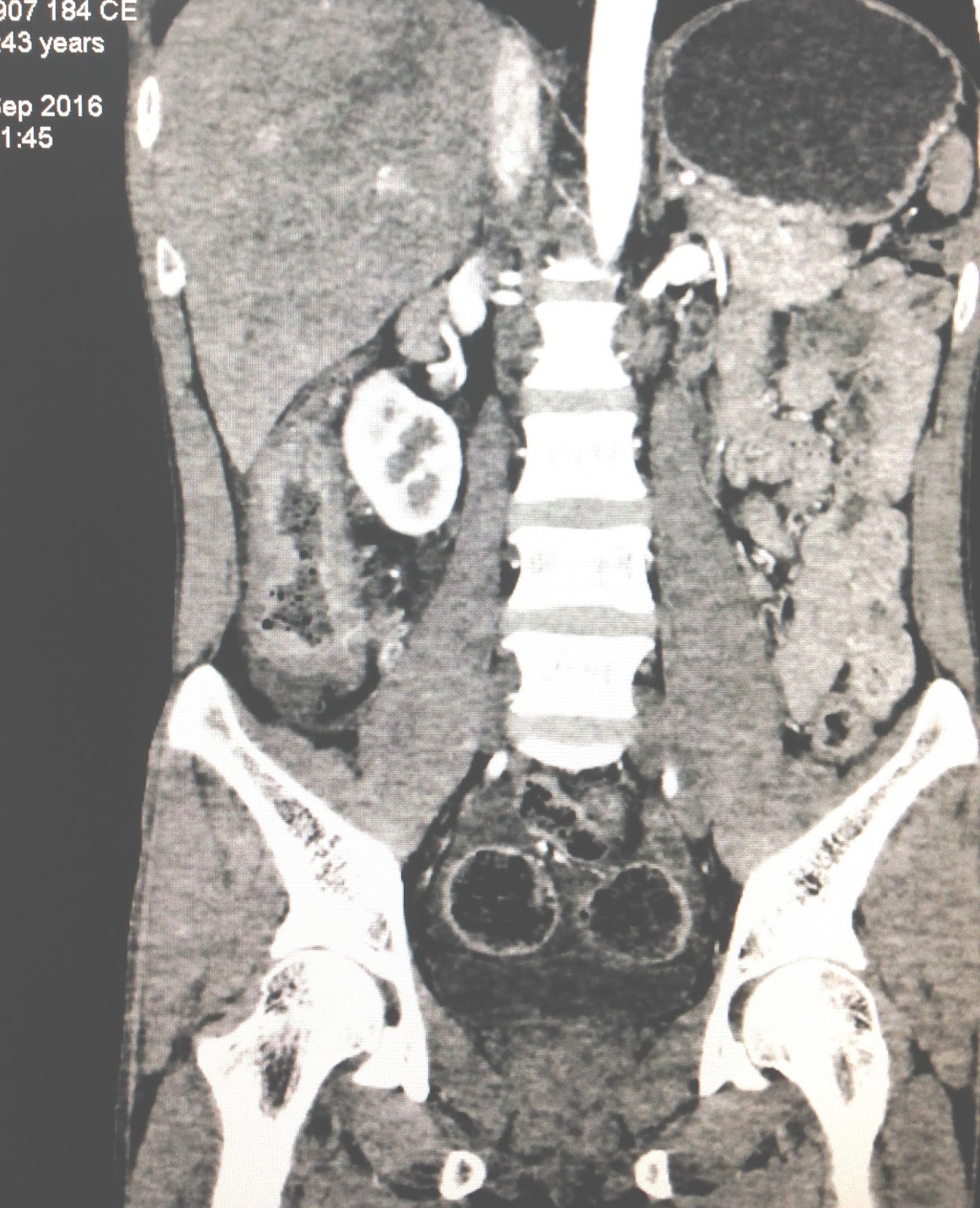
MSCT of abdomen with
CE revealed thickening of ascending colon wall (CT1,
CT2).
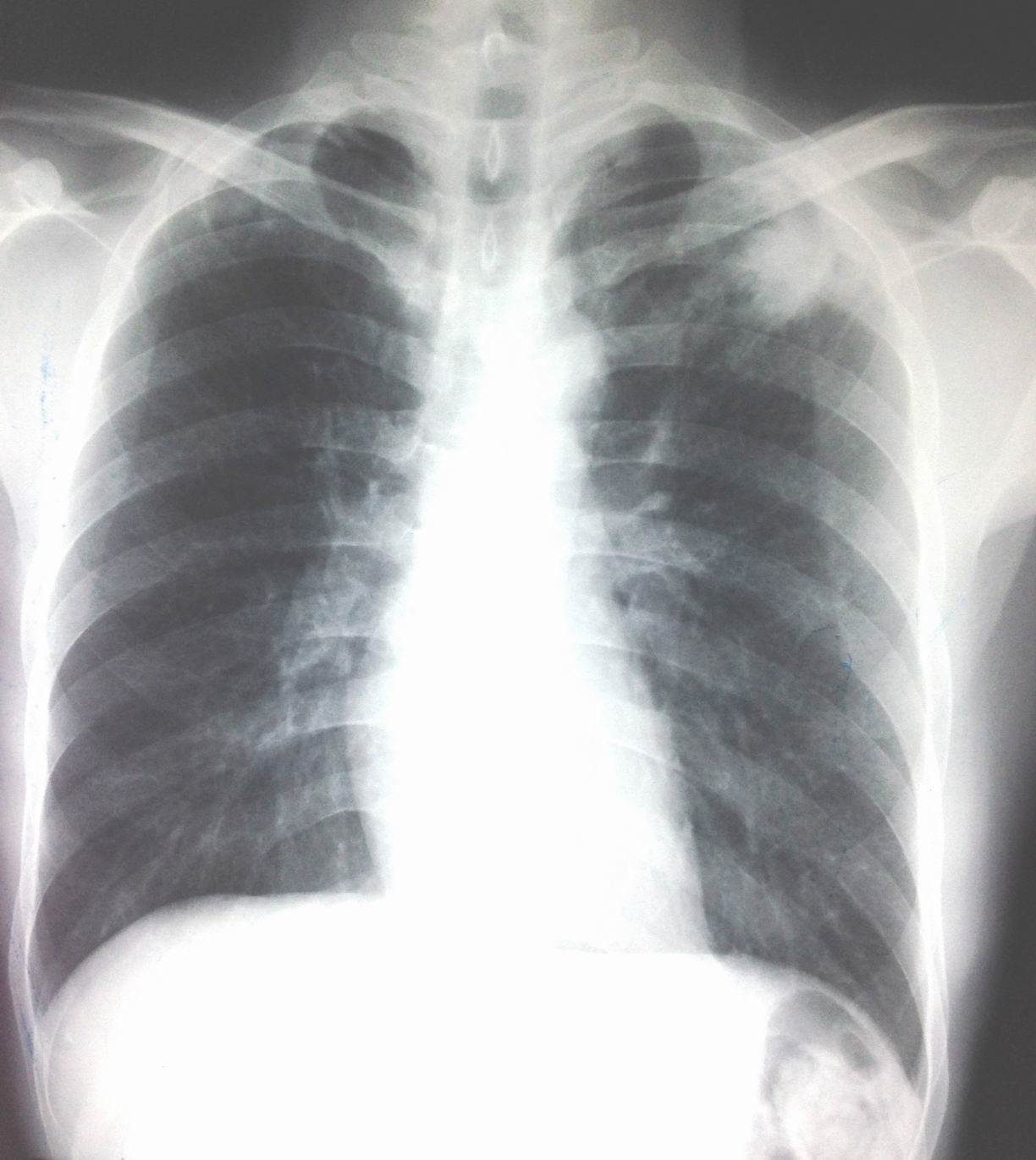
Chest X-rays before endoscopy detected infiltration of left upper lung.
Colonoscopy reported the mass in right colon, nodular ( see foto) biopsy.

Report of endoscopist is colon cancer.
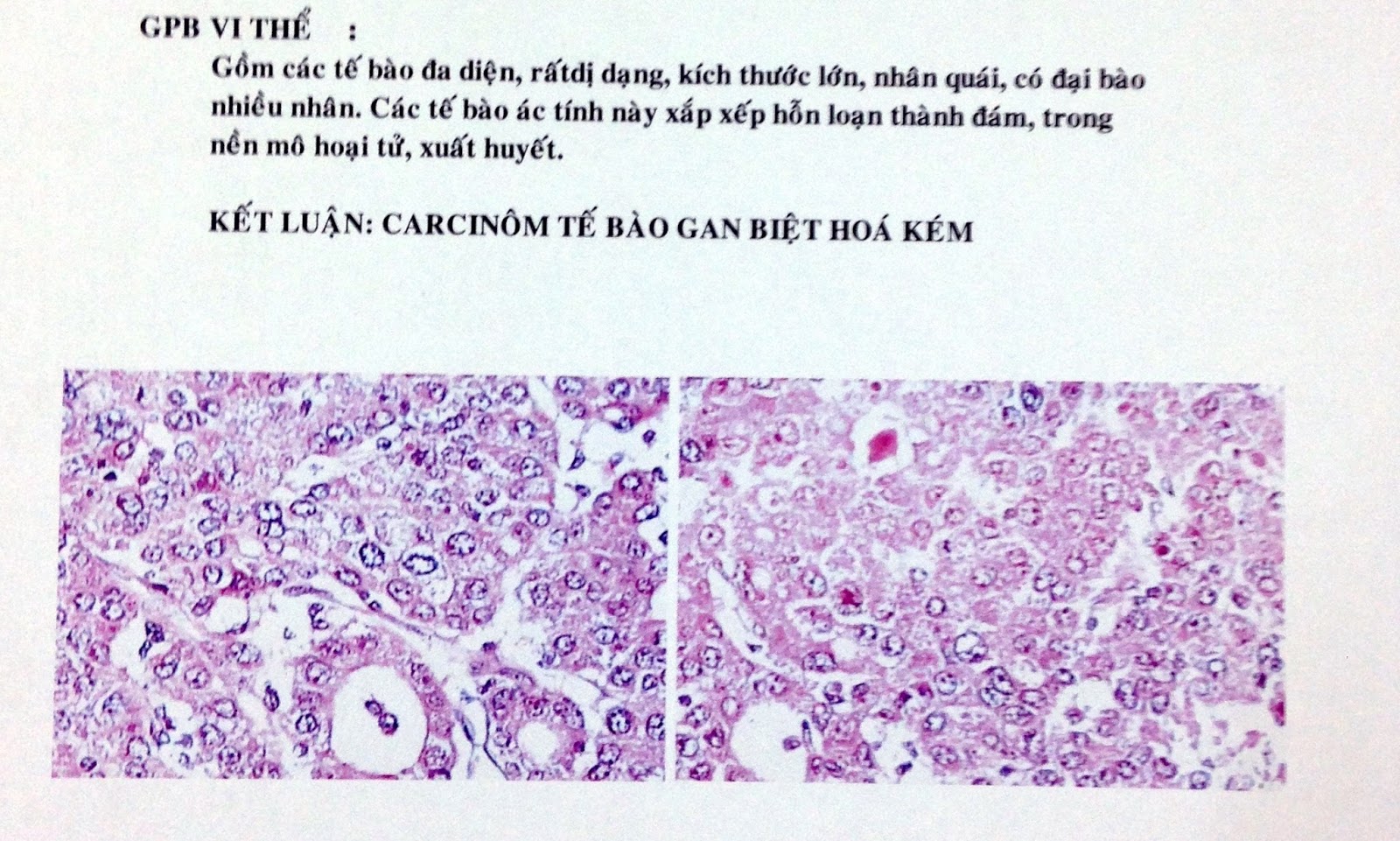
Microscopic report is colon tuberculosis.
Report of endoscopist is colon cancer.
Microscopic report is colon tuberculosis.
Conclusion = this
case represented colicky pain at epigastric region but ultrasound and CT
suggested colon cancer, same as colonoscopy, but microscopic
is tuberculosis.of colon and left lung.
REFERENCE: