
Woman 29 yo, 2 years before had been removed right leg tumor but did not to know what kind of this was, no pathology report but now she feels
shortness breathing.
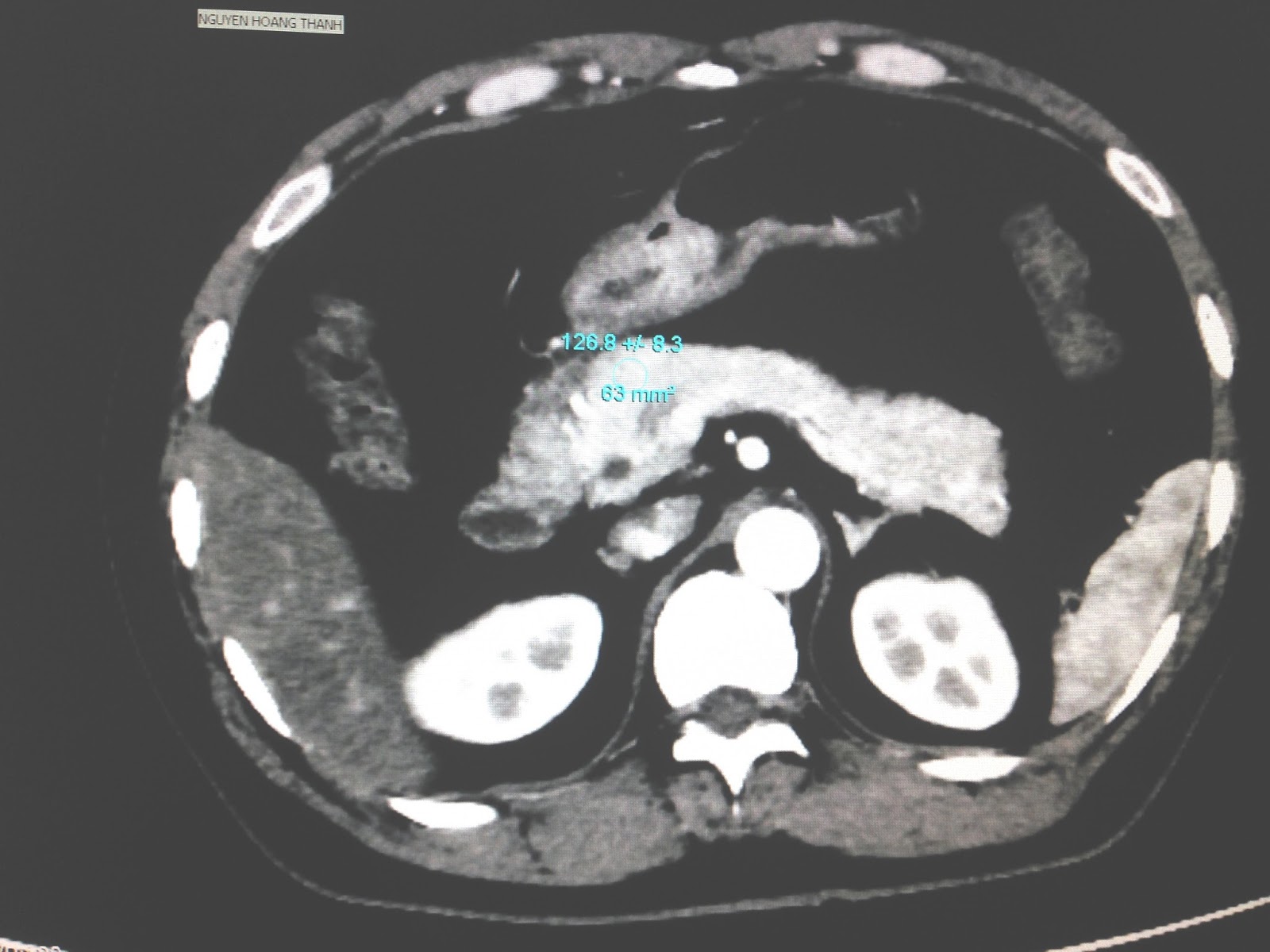
MSCT of total body detected many masses in mediastinum, left
breast, retroperitoneal
abdomen and right buttock (See CT scanning).


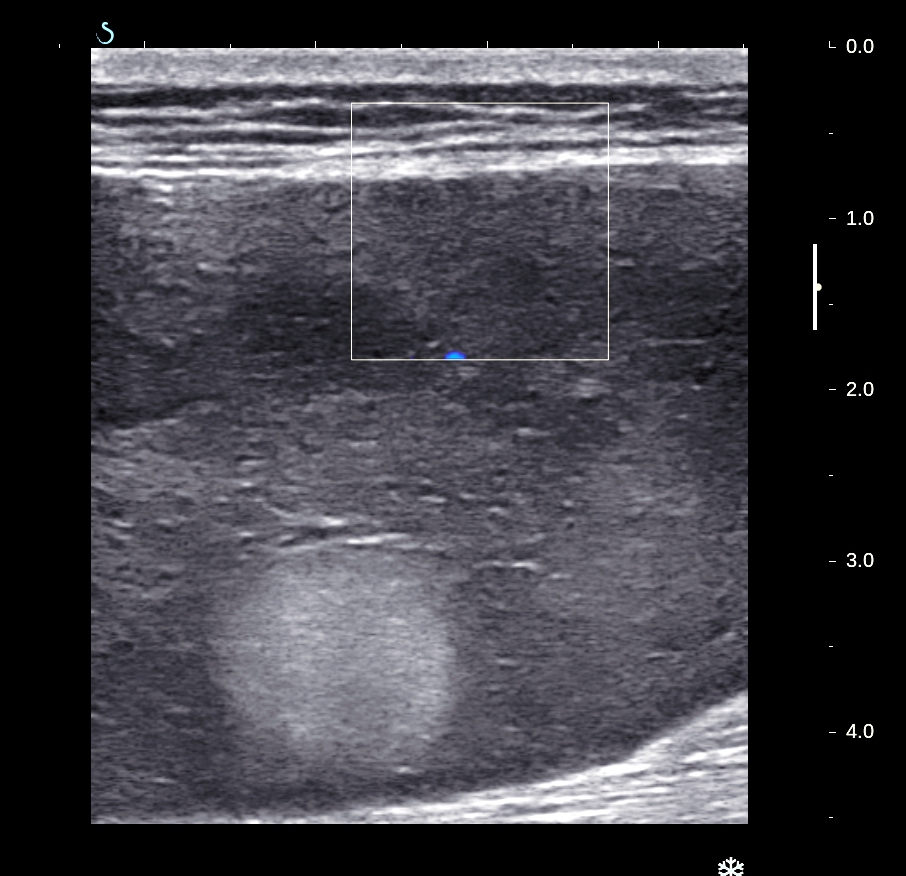
Ultrasound
scanning for verifying this mass (US1);

US 2:In epigastrum

US 3: retroperitoneum mass displaced left kidney,

US 4: mass in left breast,

US 5: mass in right buttock.
Biopsy of the mass in right buttock is
liposarcoma.

Conclusion: Multiple sites in the body of liposarcoma metastasis .
REFERENCE:

REFERENCE:










































{kind=link}