Boy 04 yo, difficulty
swallowing for 3 months. No
fever, no pain. Clinical ENT doctor’s examination
is suggestion of tonsil tumor at
right side (photo).

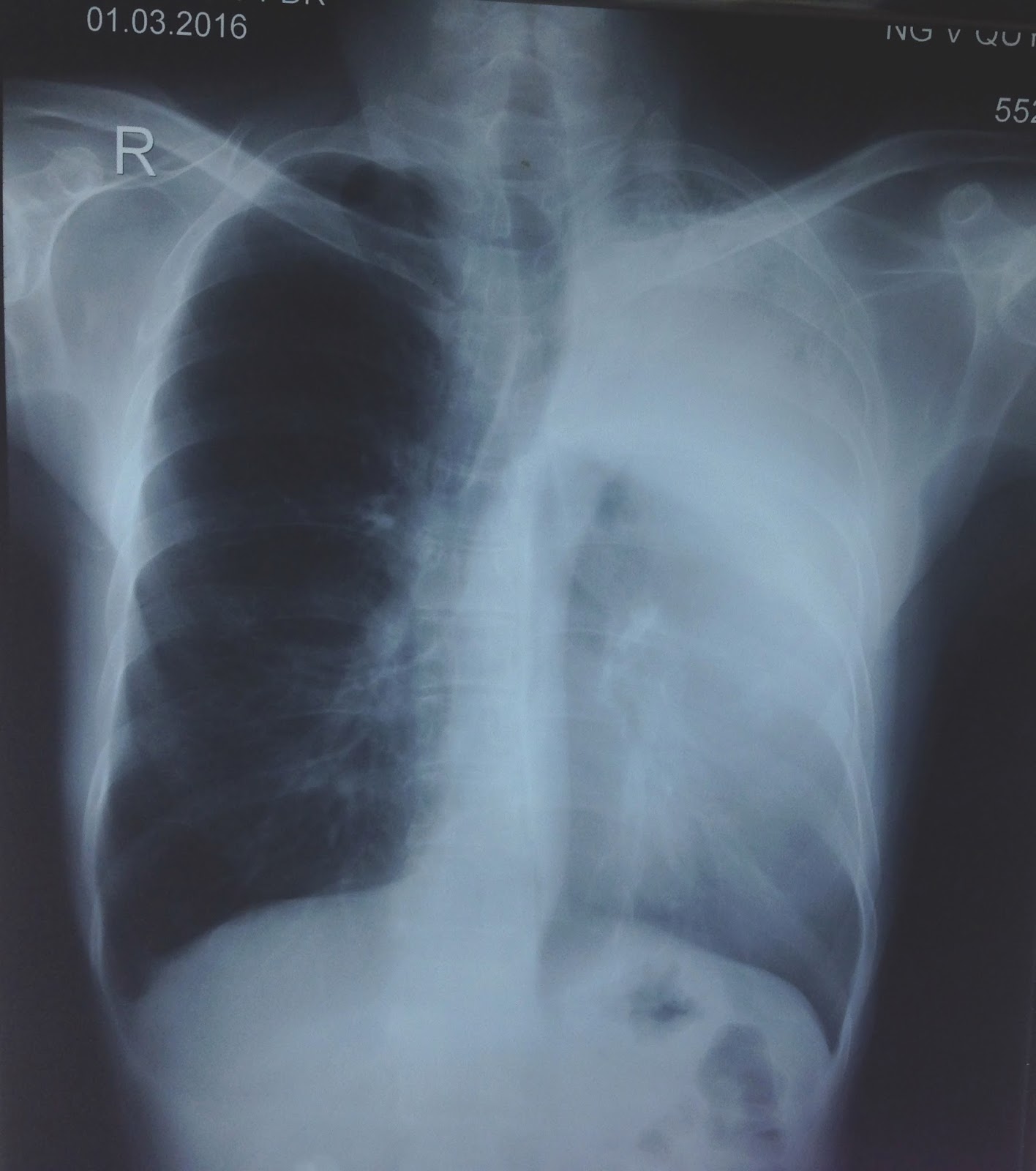
X-Rays of the neck AP and lateral view: this mass is
calcified, irregular border, precervical spinal bone, size of 4 cm ( film 1, 2)


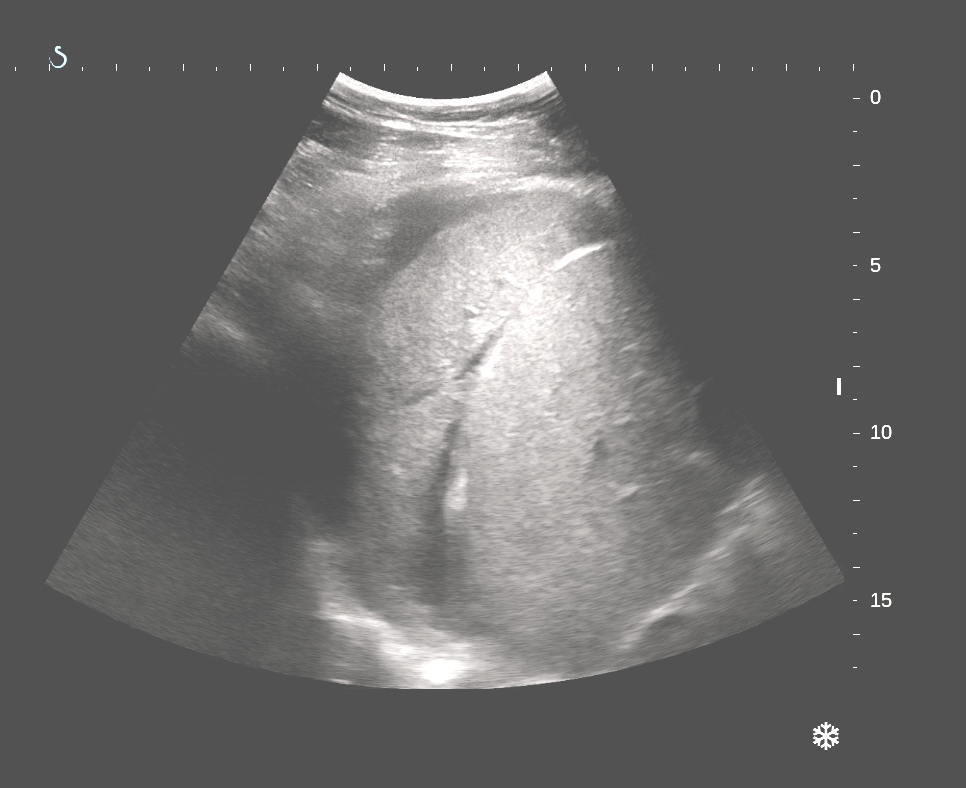
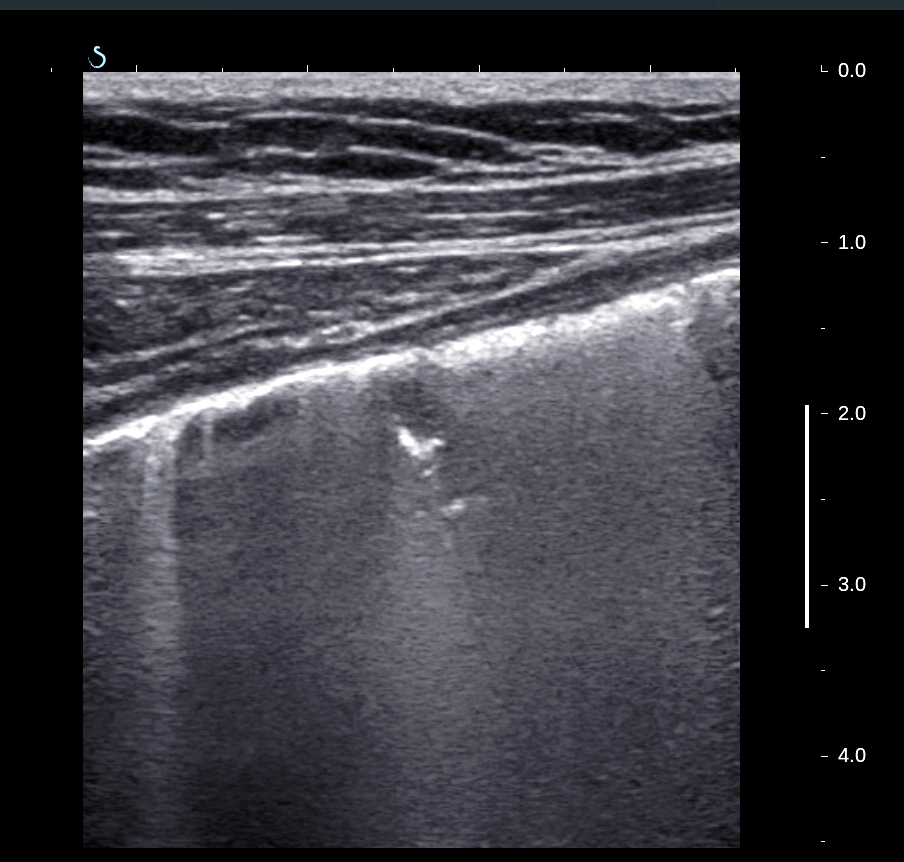
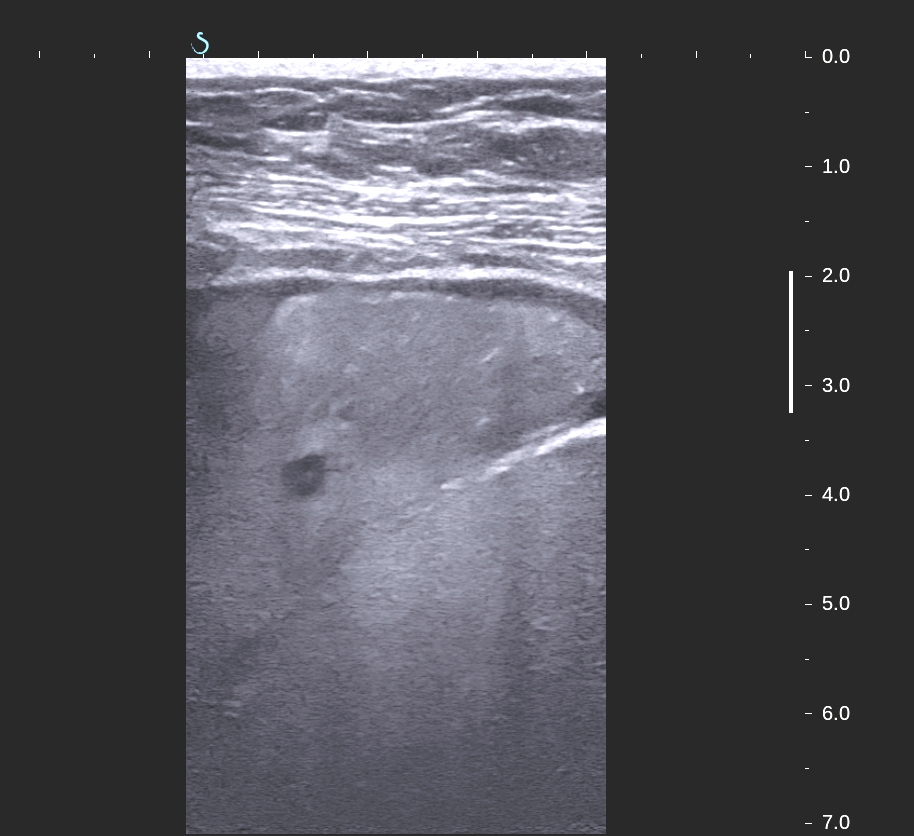
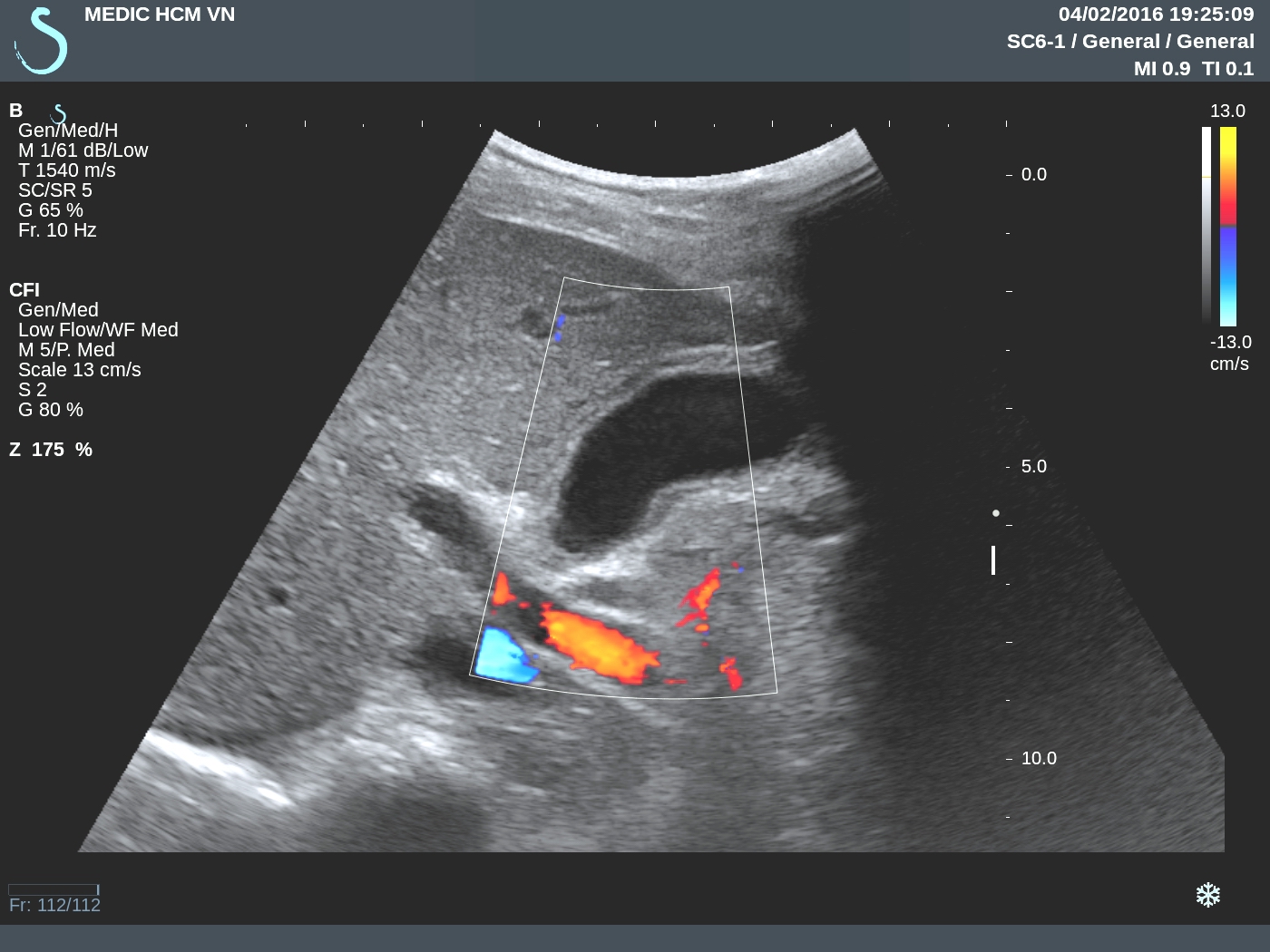
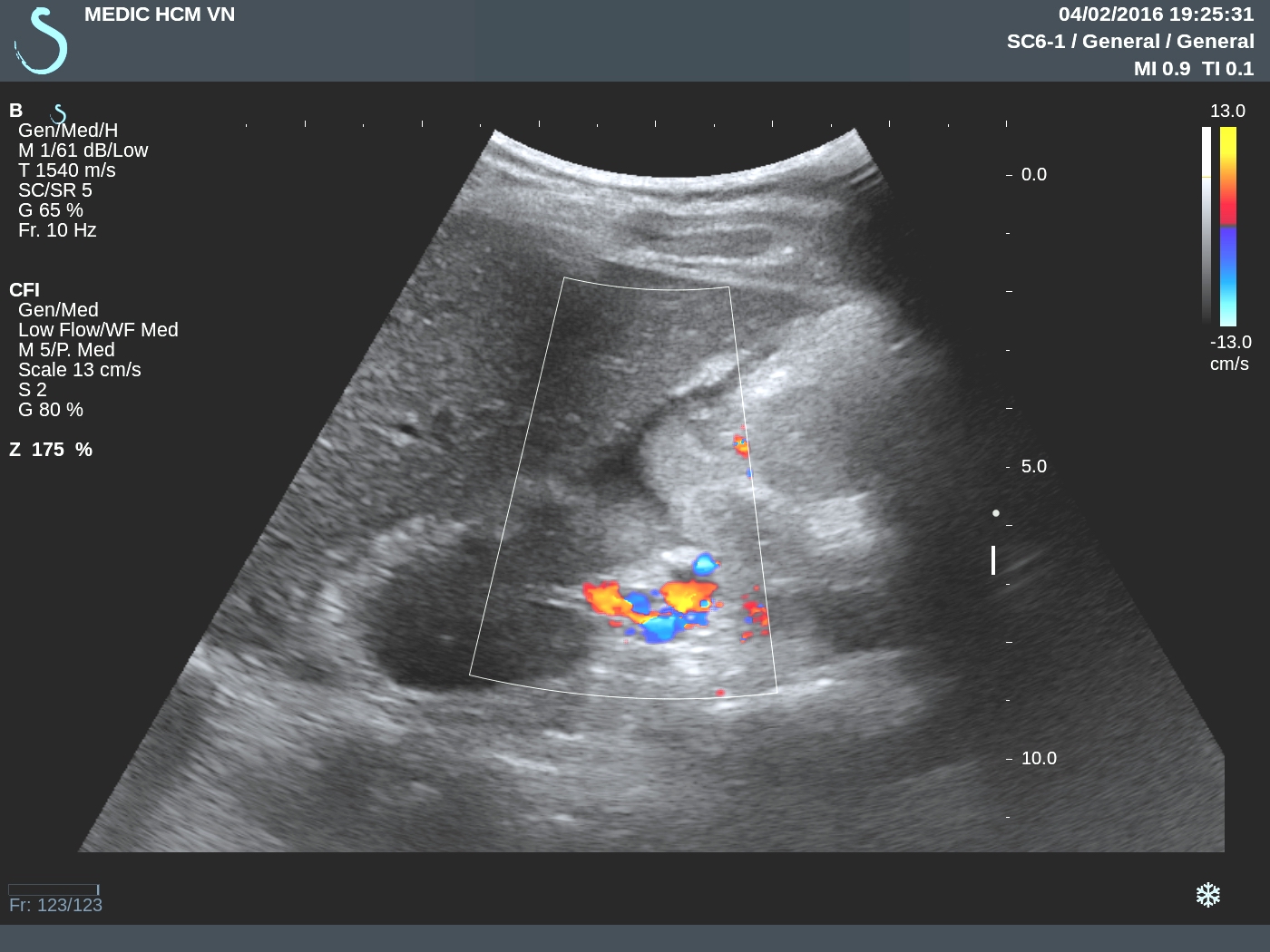
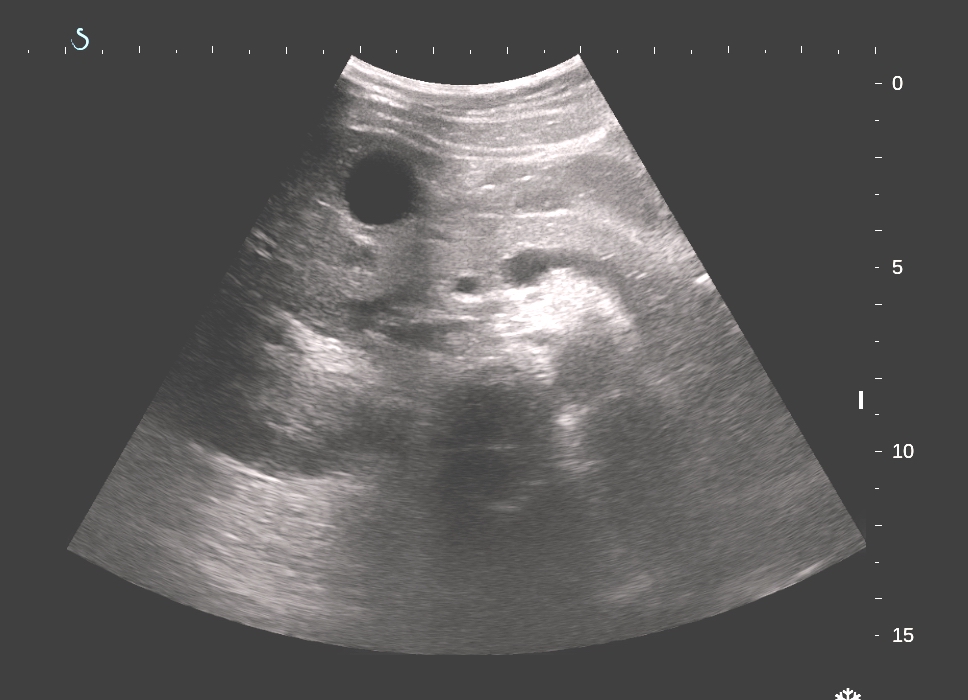
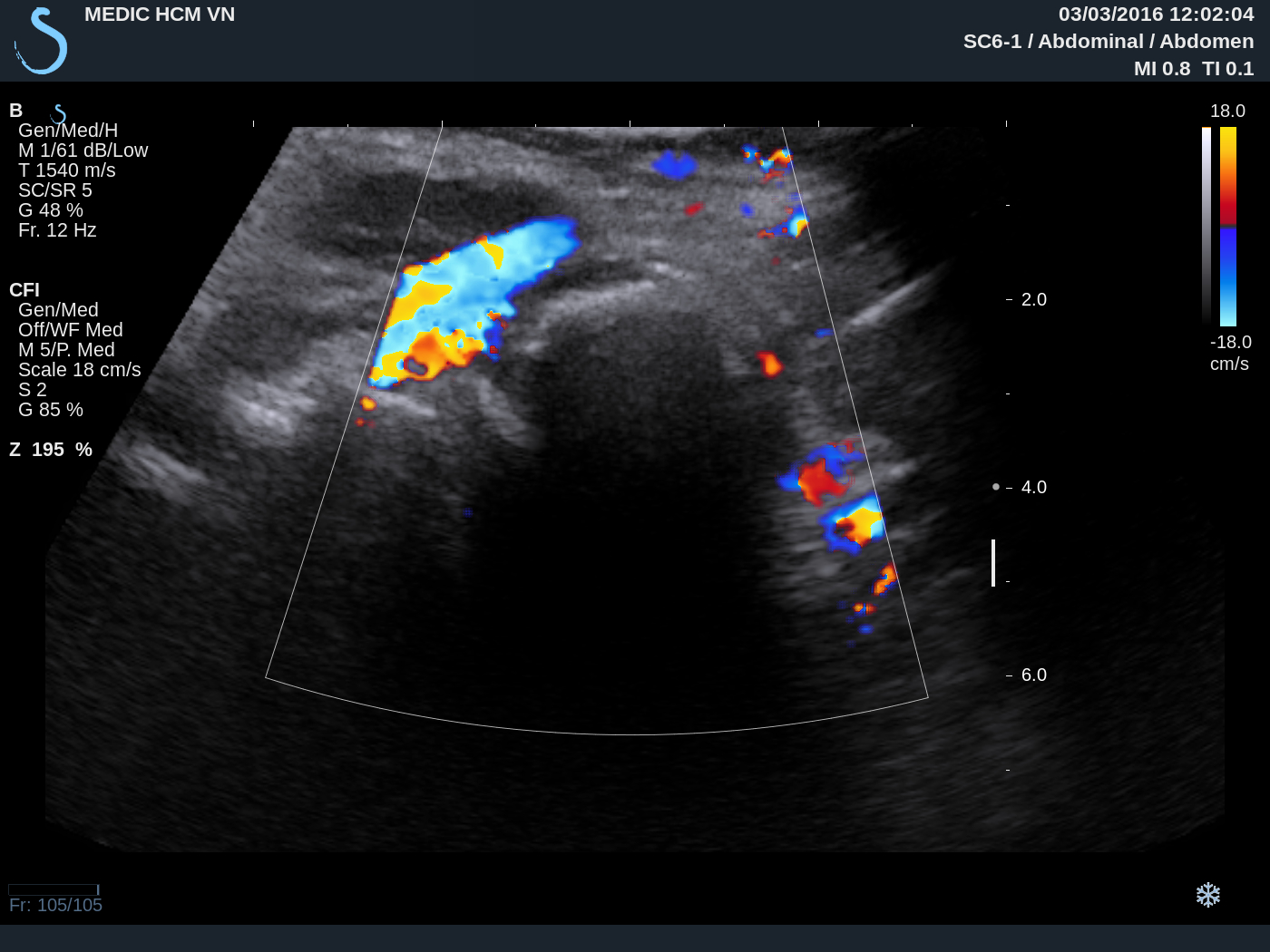
US examination of this mass:
US 1: Longitudinal scan the mass with
strong shadowing cannot inside this mass.

US 2: Cross-section view.

US 3: Relation of this mass with carotid and cervical spinal bone.
CT scan= CT 1:sagittal view , CT 2: cross- section with PA view, CT3: cross-section with AP view.



Based on clinical, X-Rays , ultrasound and CT, what is your diagnosis?
Based on X-Rays and CT some doctors suggested teratoma of oropharynx, or enchondroma.



Based on X-Rays and CT some doctors suggested teratoma of oropharynx, or enchondroma.
MRI ( 2 pictures sagittal and section) radiologist diagnosis is chondroma.
Operation today removed one hard mass looked like stone.
Microscopic report of this mass is fibrous dysplasia ossificans progressiva which is same as myositis ossificans
 REFERENCE : case report.
REFERENCE : case report.

Microscopic report of this mass is fibrous dysplasia ossificans progressiva which is same as myositis ossificans