A 26 year-old female patient who had complained
mild pain at her pubic region presented lower abdominal pain a
month prior. She overwent a caesarean
section a year ago for delivery her child.
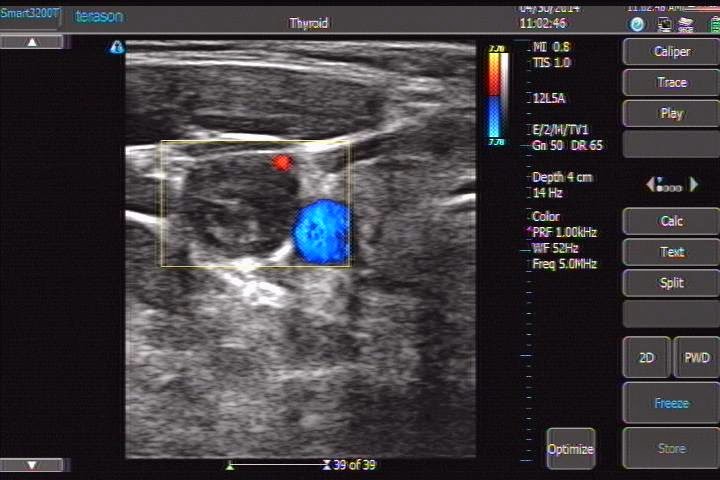
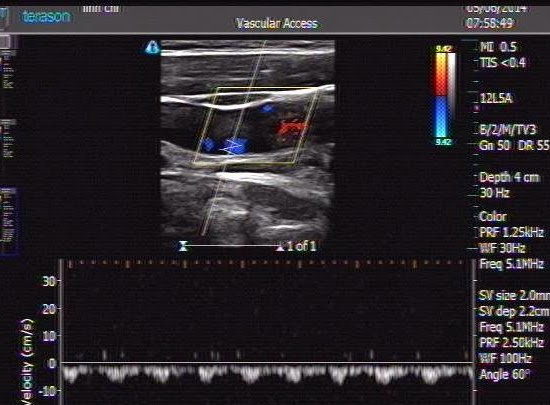
Ultrasound findings:A cystic mass (about 83x46 mm) containing distinct internal hyperechoic wavy, striped structures.



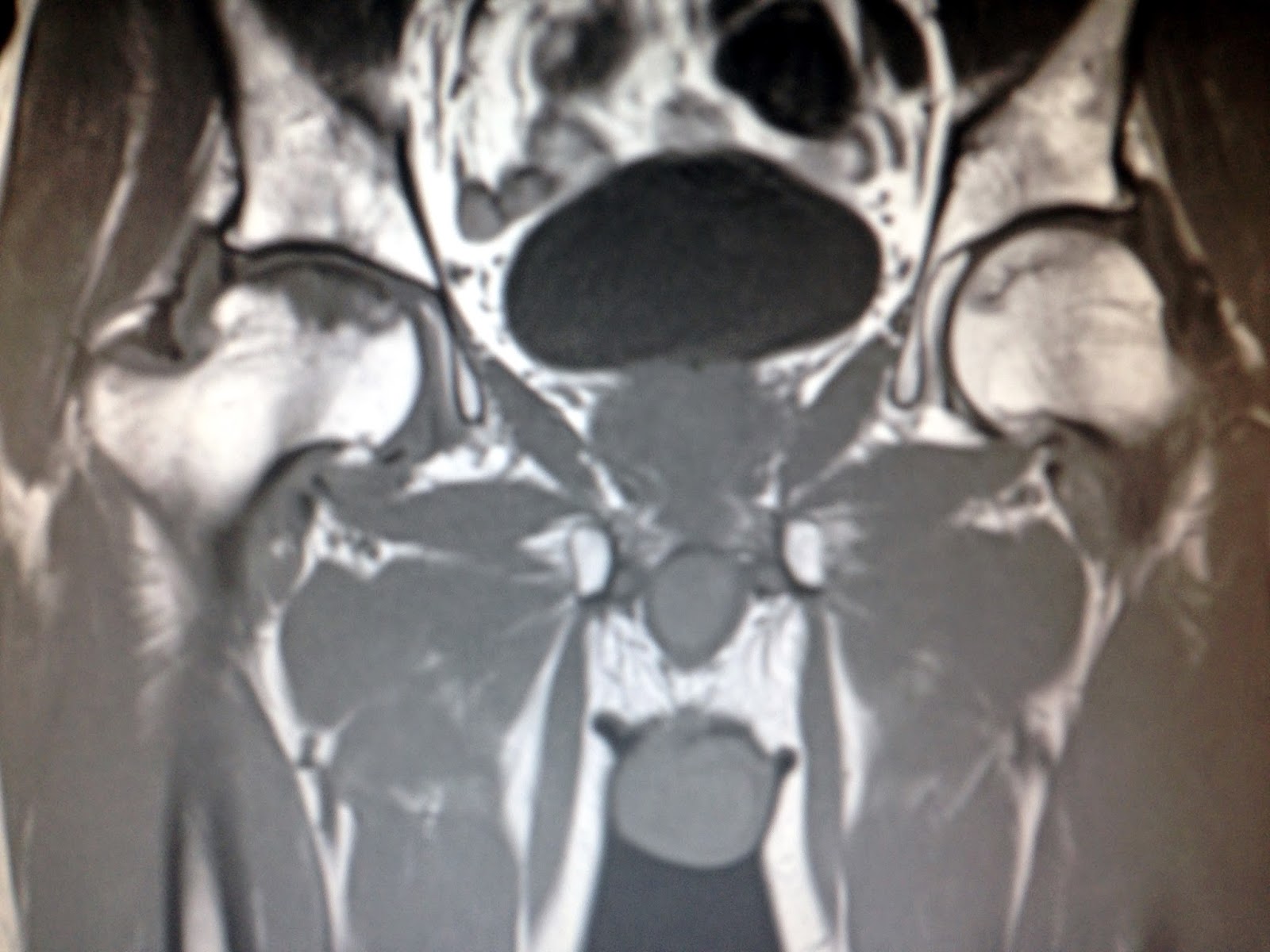
CT Scan abdomen: A mass of 11 x 9 cm with
thicken enhancing walls was seen in pelvis.



But diagnosis of gossypiboma
was made and at laparotomy: a surgical sponge (18x22 cm) with adjacent
inflammatory tissue and pus were removed successfully.


DISCUSSION:
A diagnosis of gossipiboma pre-op seems to be very difficult
that always need skill and experience. Because of imaging findings of gossypiboma are
nonspecific and complexe so the right diagnosis in pre-op is still acchived about 1/3 of
cases in literature.
But whenever an unknown mass into abdomen with exist surgical scare that should dissolve it may be a gossypiboma or not.