Man 27 yo, dental
pain on right mandibular for one week, he detected the right side of neck along SCM muscle getting hot and swelling, pain
and fever (see photo).

He was treated with antibiotics and went to
ultrasound scanning. Sonologist detected
this neck mass beeing
like abscess by fluid collection on right and left neck (see 3 photo and video).



MSCT found out the right mass along SCM muscle and one other mass on left side nearby thyroid
gland.



Puncture this mass removed the pus but direct examination with gram stain no bacteria.
Operation for drainage.


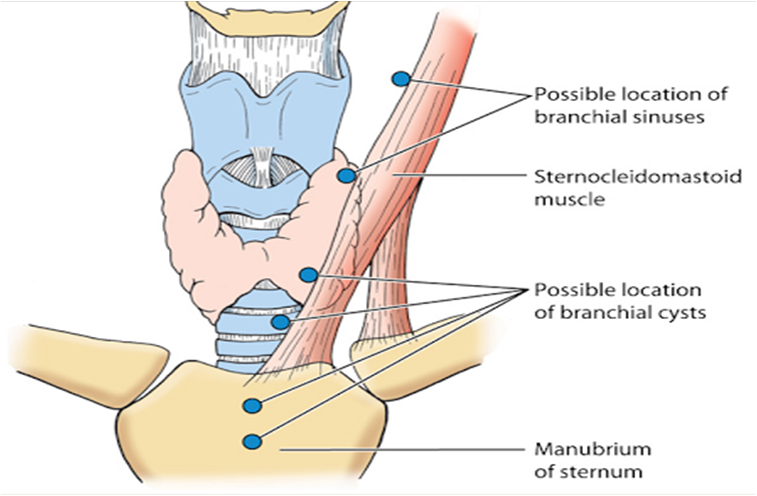
DISCUSSION: IT IS A CYST of INFECTION at LATERAL SITE OF THE NECK. THE MOST COMMON IS BRANCHIAL CYST.
CT ALSO SUPPORTED THIS DIAGNOSIS.
REF..ANATOMY OF BRANCHIAL CYSTS.