Woman, 20 yo, discovered HTA in pregnant at 16 weeks
5-months before this hospitalization:
pregnant in 28ws, sudden obstetrical seizures in Ca Mau hospital. Diagnosis of eclampsia / hypertension / 28w
pregnant. Treatment: cesarean section.
After surgery ,
patients changed body shape, round, fat
face, neck, stretching skin, increasing weight gain, examination findings adrenal
gland tumor in Can Tho General Hospital,
then transferred to Binh Dan hospital.
In clinic examination, obesity, Cushing syndrome, other organs
detect no abnormalities. HTA being
treated.

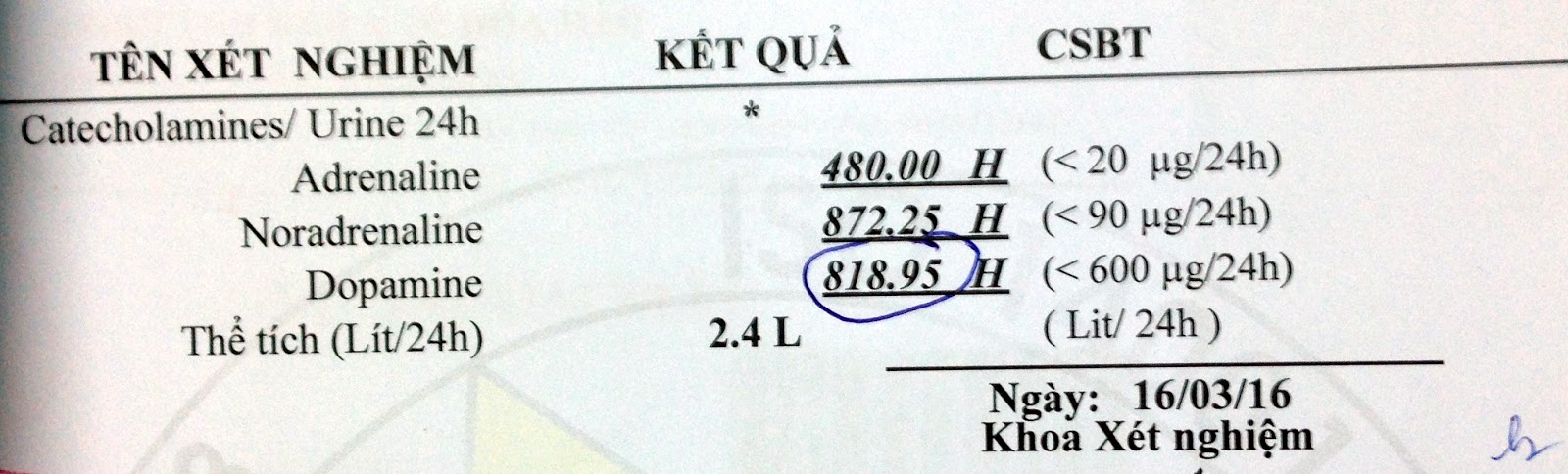
Blood and urine catecholamine increasing, blood and urine
cortisol increasing, ACTH reducing.

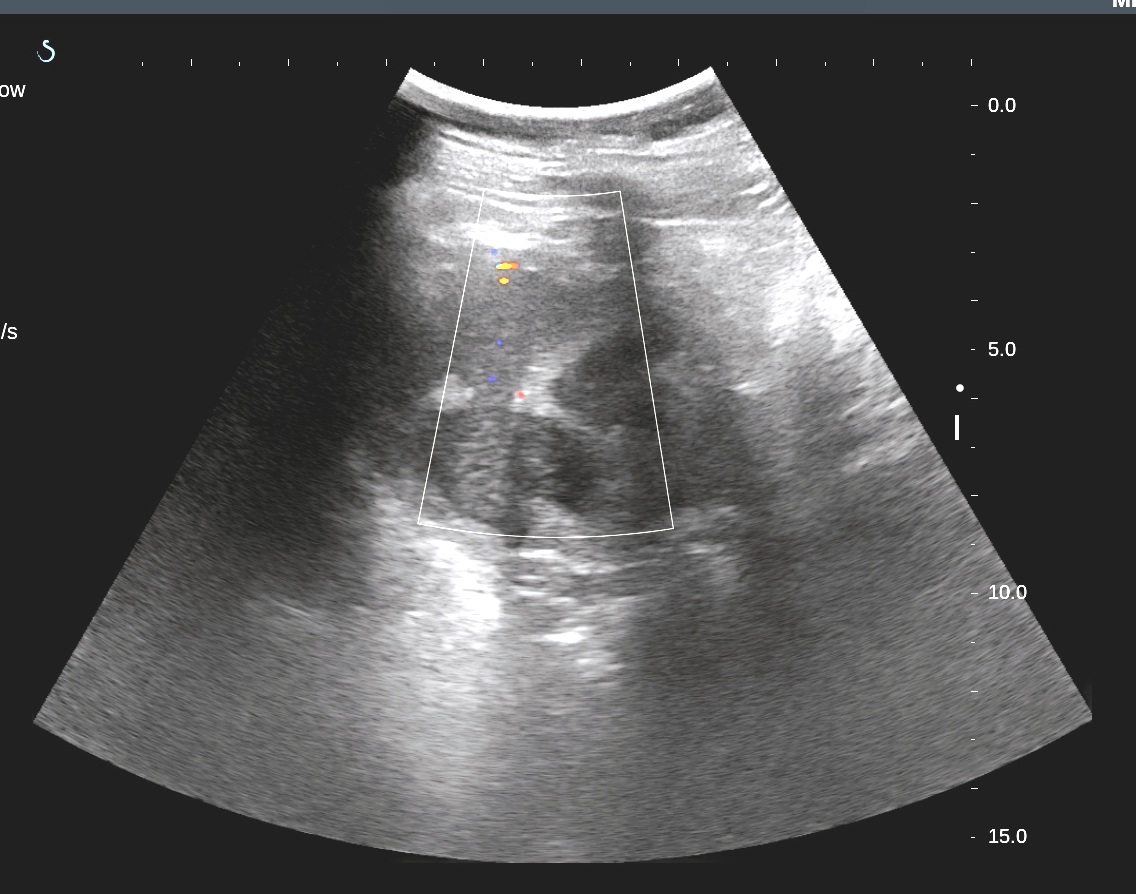
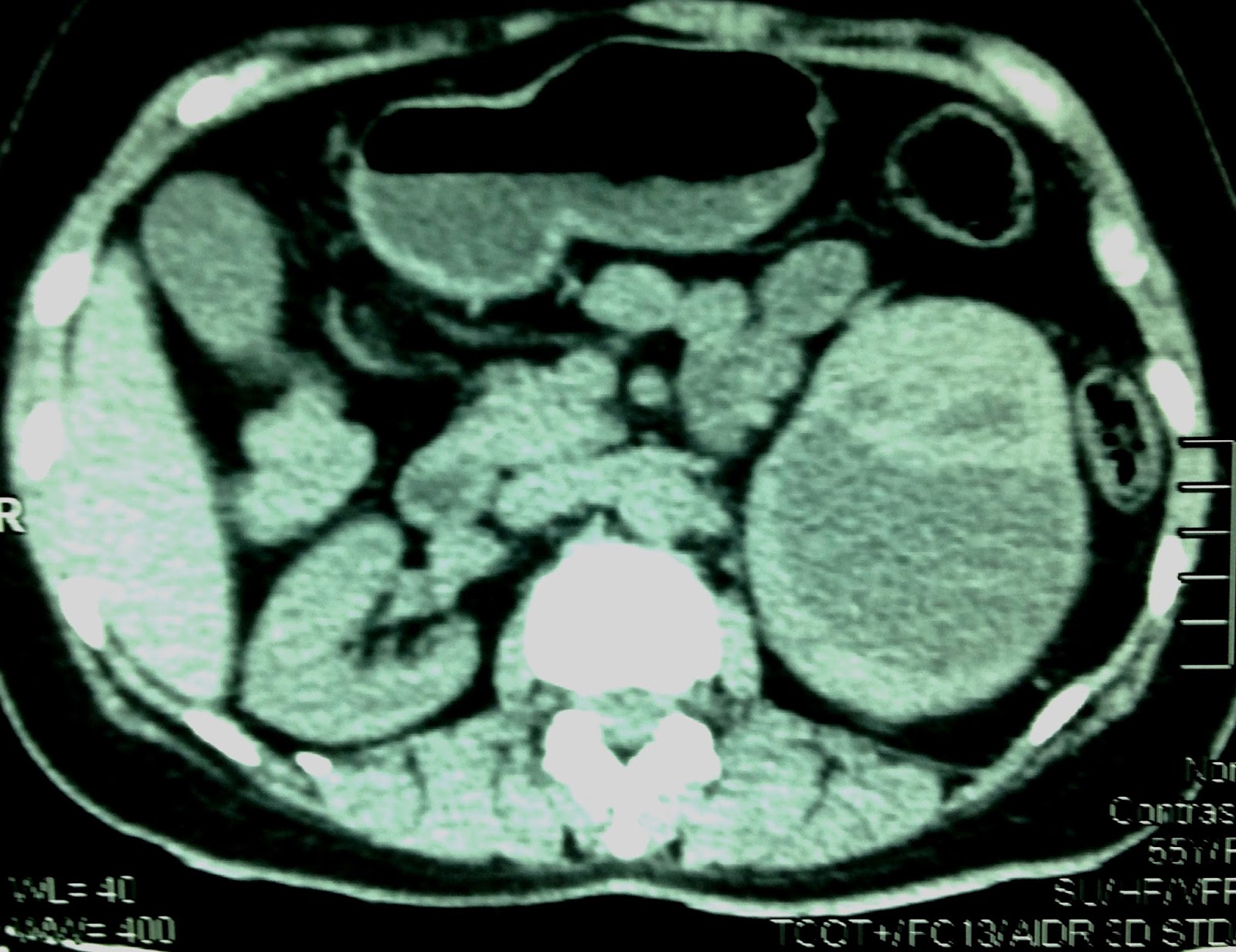
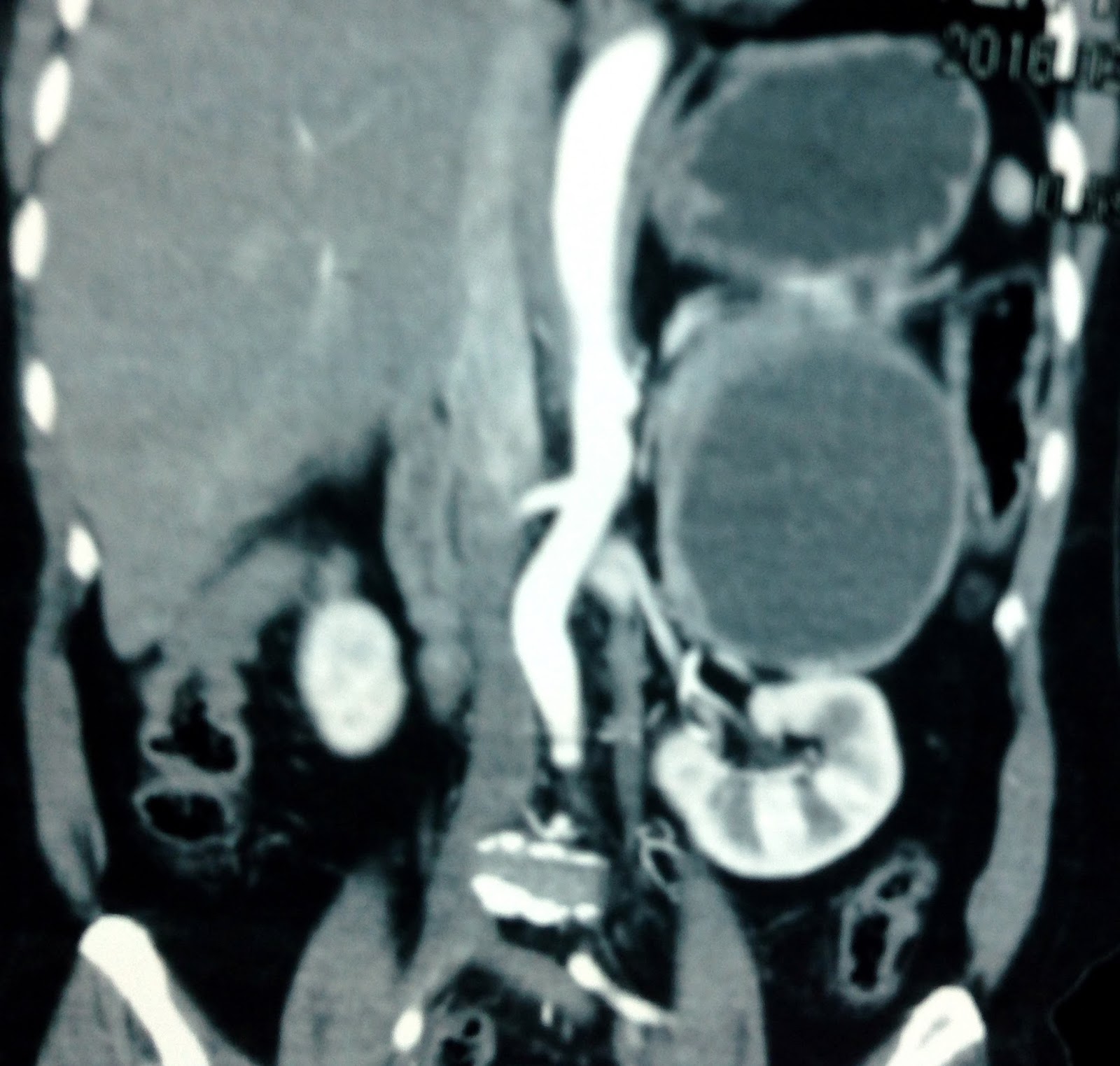
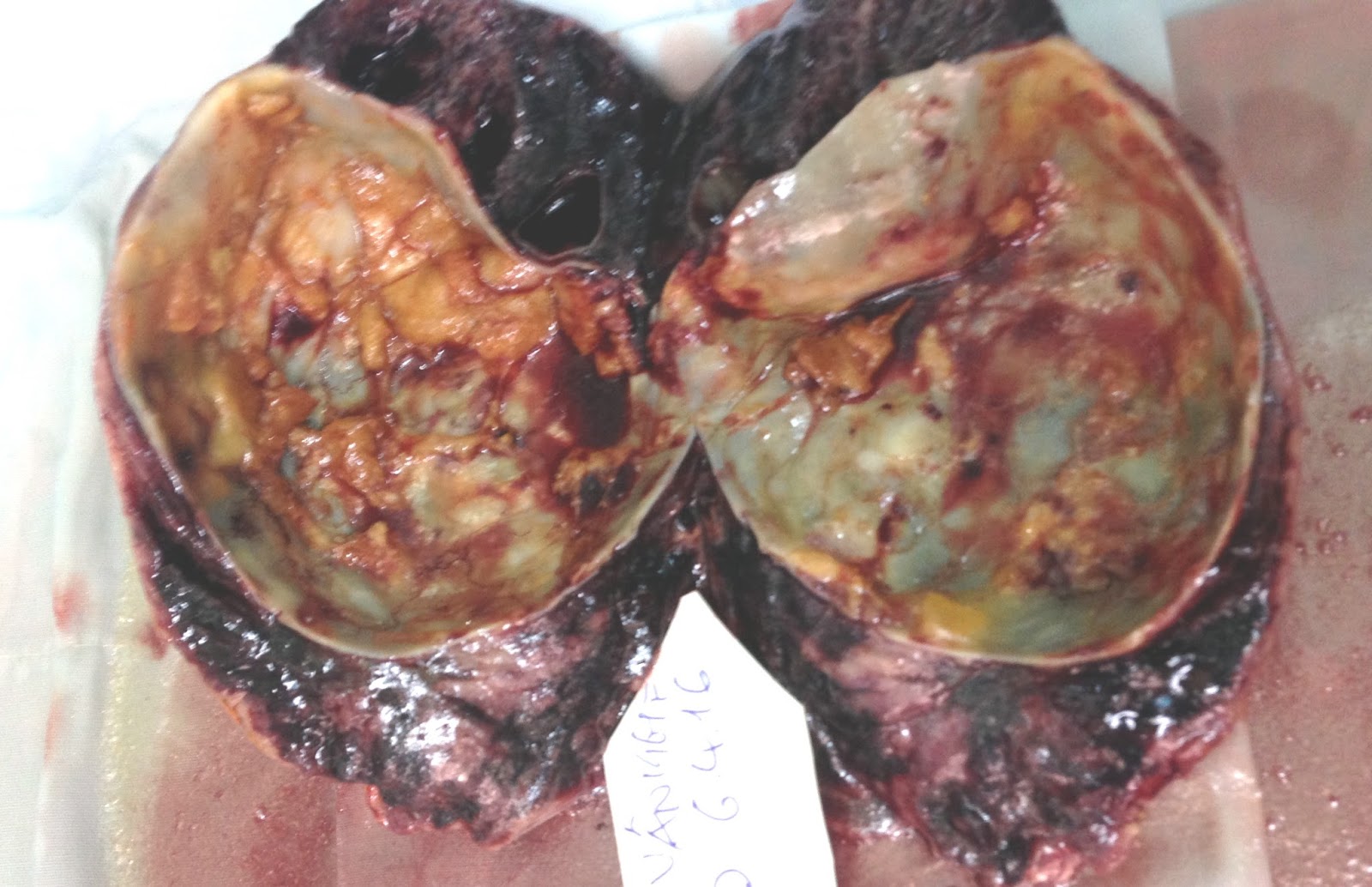
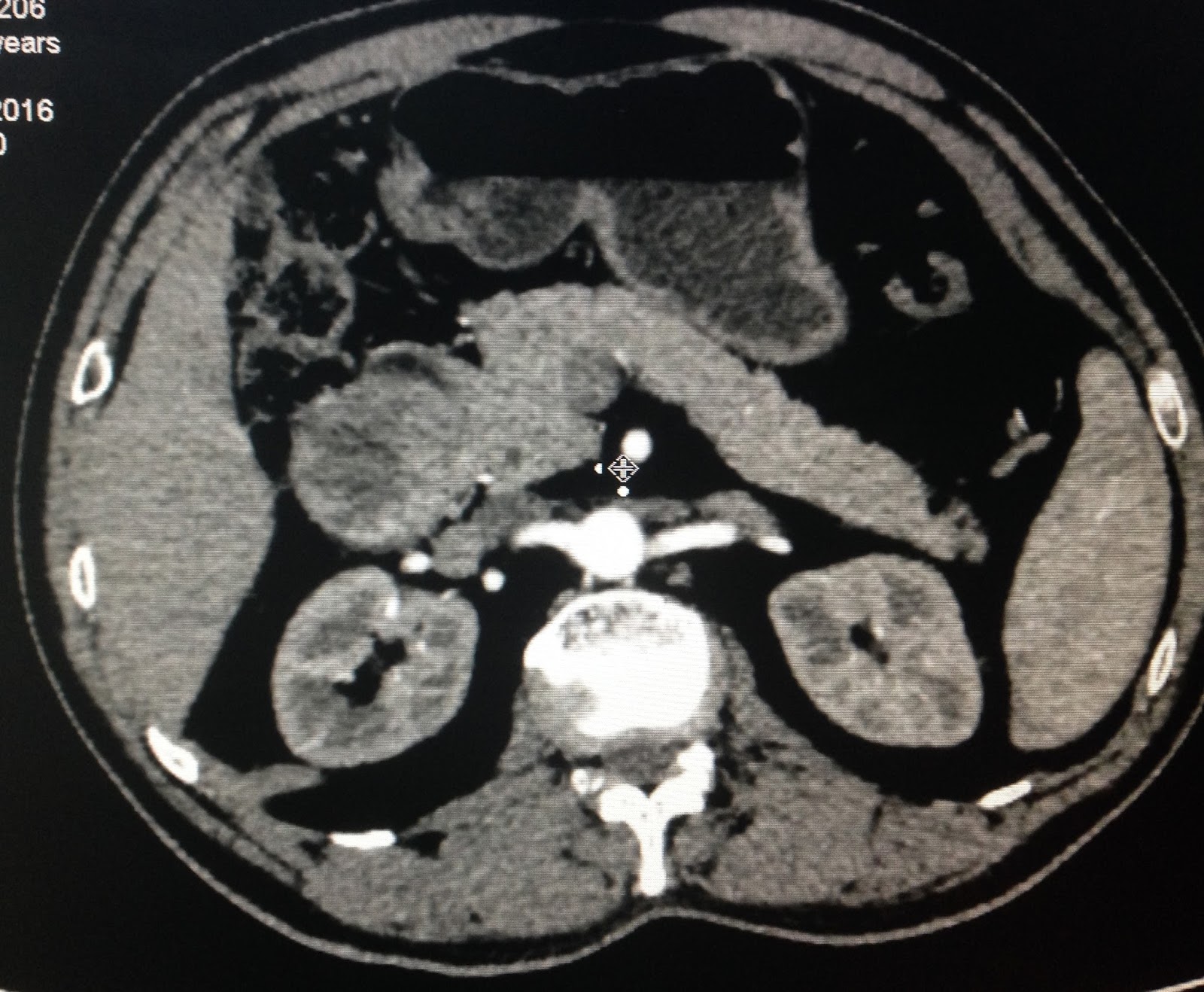
MSCT: right adrenal tumor.
CONCLUSION= Female patient 20 yo, hospitalized for weight gain and HTA, Cushing syndrome. Reducing of blood ACTH and metanephrine; catecholamine and cortisol secretion increasing in blood, and urine.
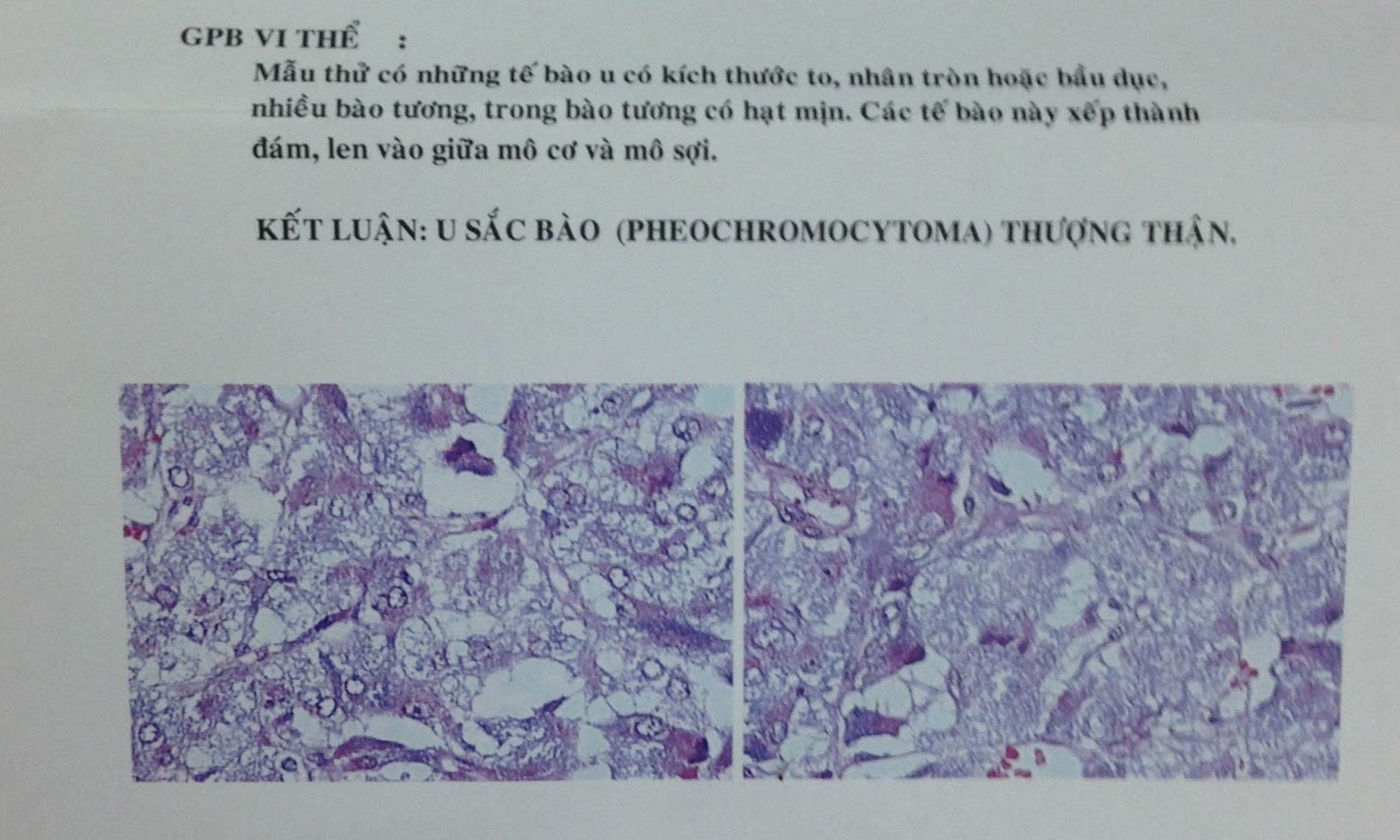
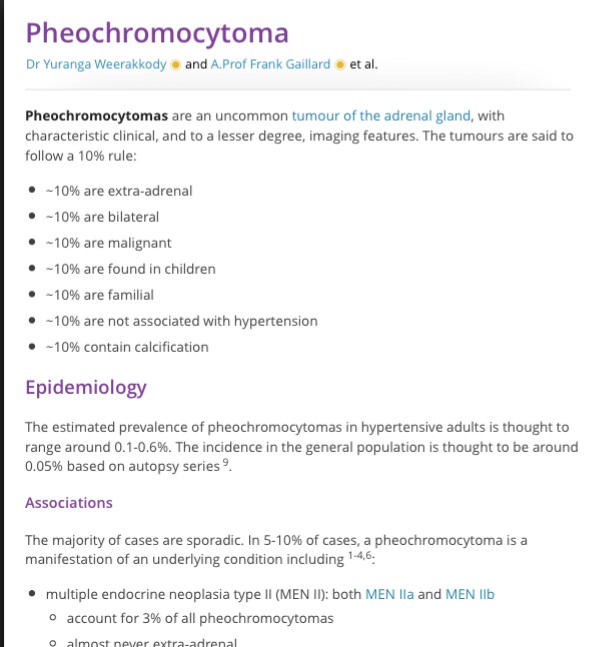
Surgery removed right adrenal tumor. Pathological result is malignant pheochromocytoma.

Secreted adrenal neoplasms - suppression of axis of adrenal
pituitary.