Female patient 82 yo, herself detected a right breast mass that had been in traditional management, but it was getting slowly bigger. Now the right breast is swollen and hemorrhage.
Ultrasound detected tumors at right and left breast. Noted BI-RADS 5 with metastase lymph nodes of right breast tumor, and BI-RADS 4A for the left one.
Ultrasound findings:
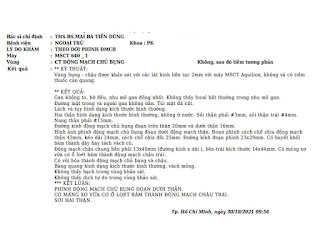
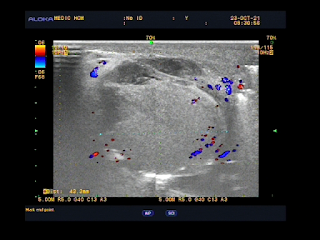
Right breast = Lesion with mass effect is at 1/2 lateral breast, heterogenous, multiloculated, solid inside with multicalcified foci and neoplastic vessels. Limits of right pectoralis muscle and the lesion is not clear. This lesion invades subcutaneous fatty tissue and right breast skin . Because of big size tumor it can not examined posteriorly the breast tumor.
Left breast= Many cystic structures with calcified foci, the biggest one is at 3 o'clock and far from center about 3 cm.
Many lymph nodes loss hilus with microcalcification exist in axillary areas both 2 sides and in right supraclavicular fossa.
Comet tail artifacts at the lung base both 2 sides.
MSCT with CE also detected right breast tumor and lymph nodes.
CT= Right breast lesion is heterogenous tissue condensation, multiloculated invades breast skin and deformes right breast, highly captured CE, # 61.3 x 80.2mm. Some right axillary lymph nodes # 11mm. There is pulmonary fibrosis and pleural thickening at the right lung base.
Wait for surgery.