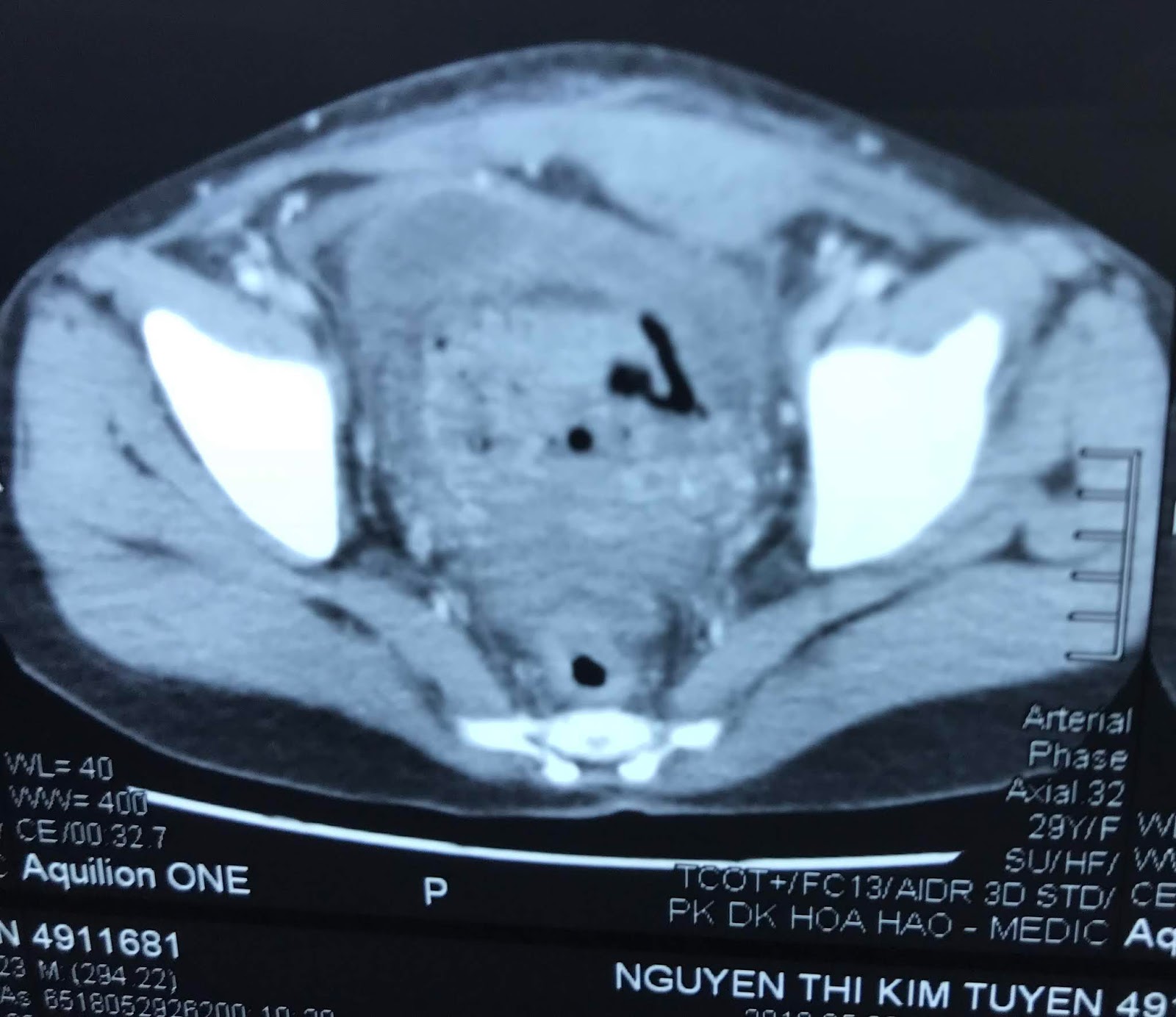
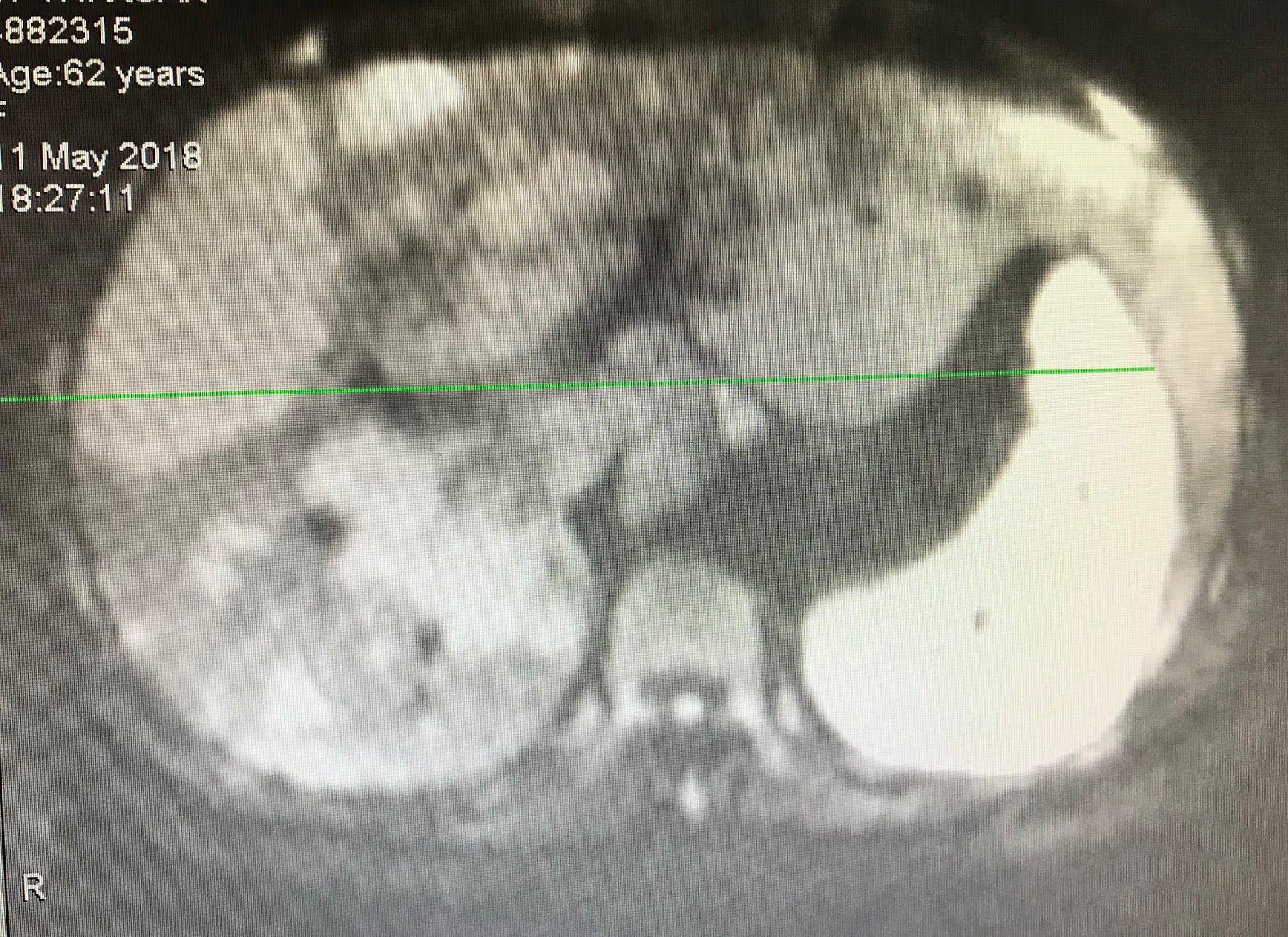
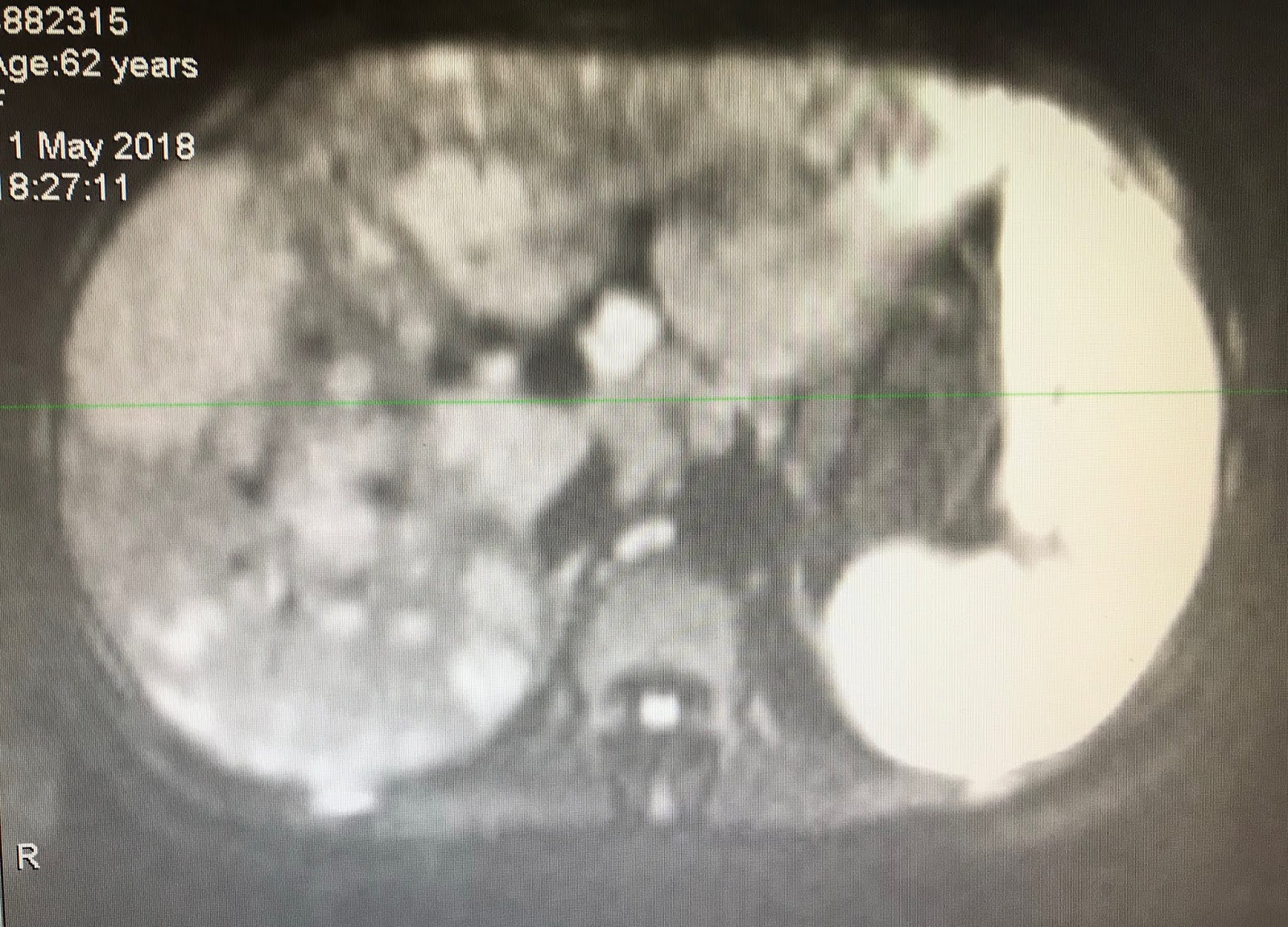
Man 47 yo with pain at RLAQ at palpation looked like appendicitis and skin of right leg inflammed red and bulleous growth with multiple nodules.( see photo of abdomen and leg skin).


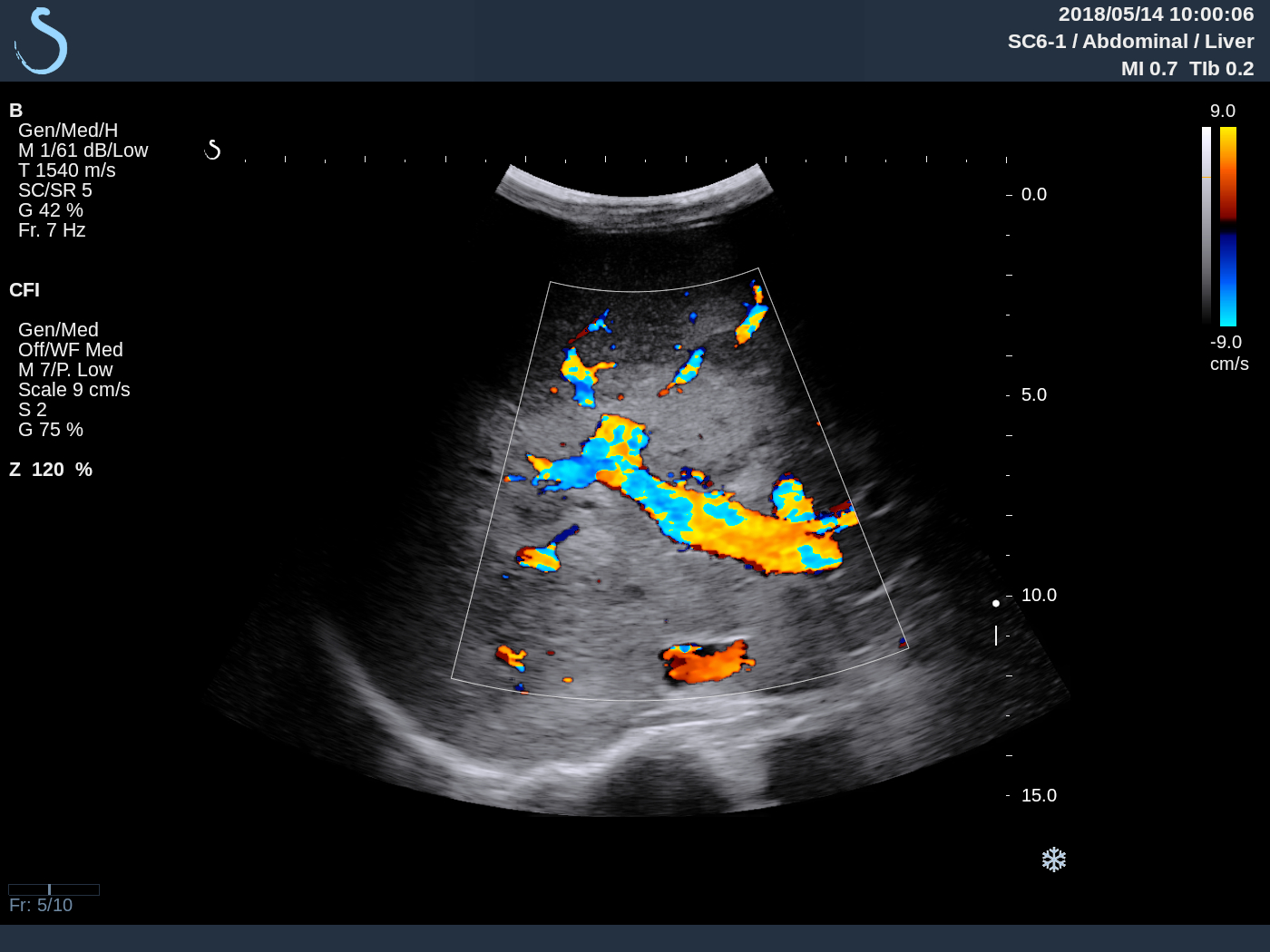
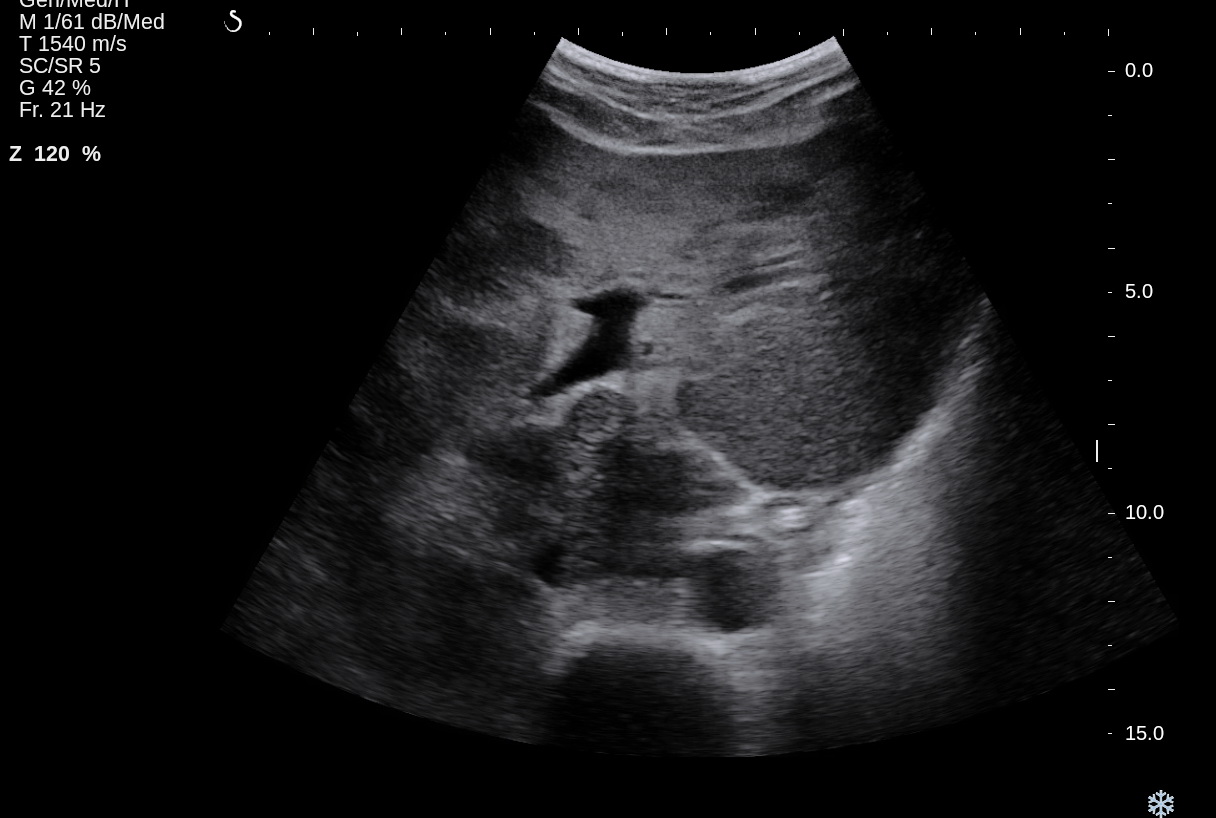
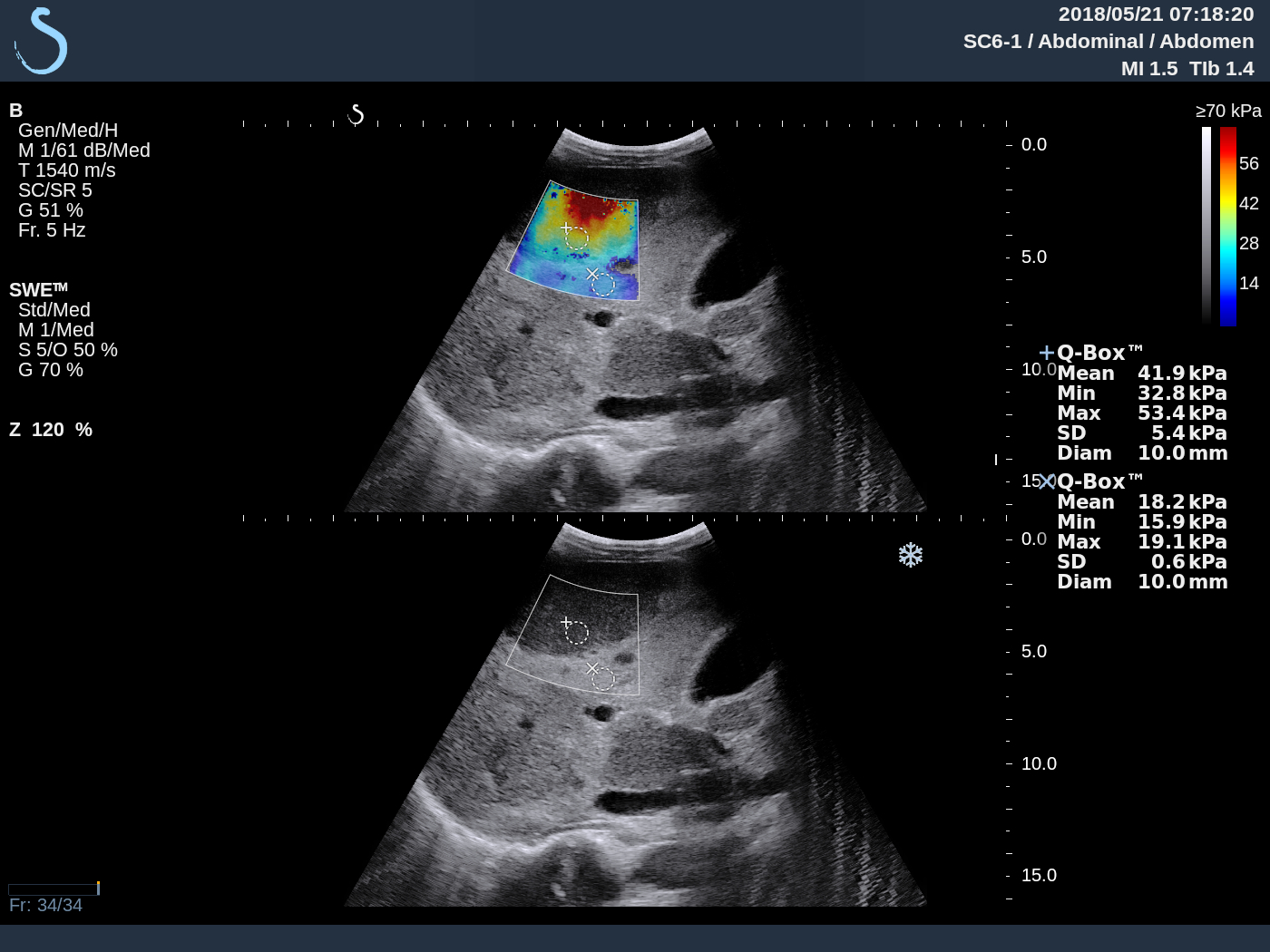
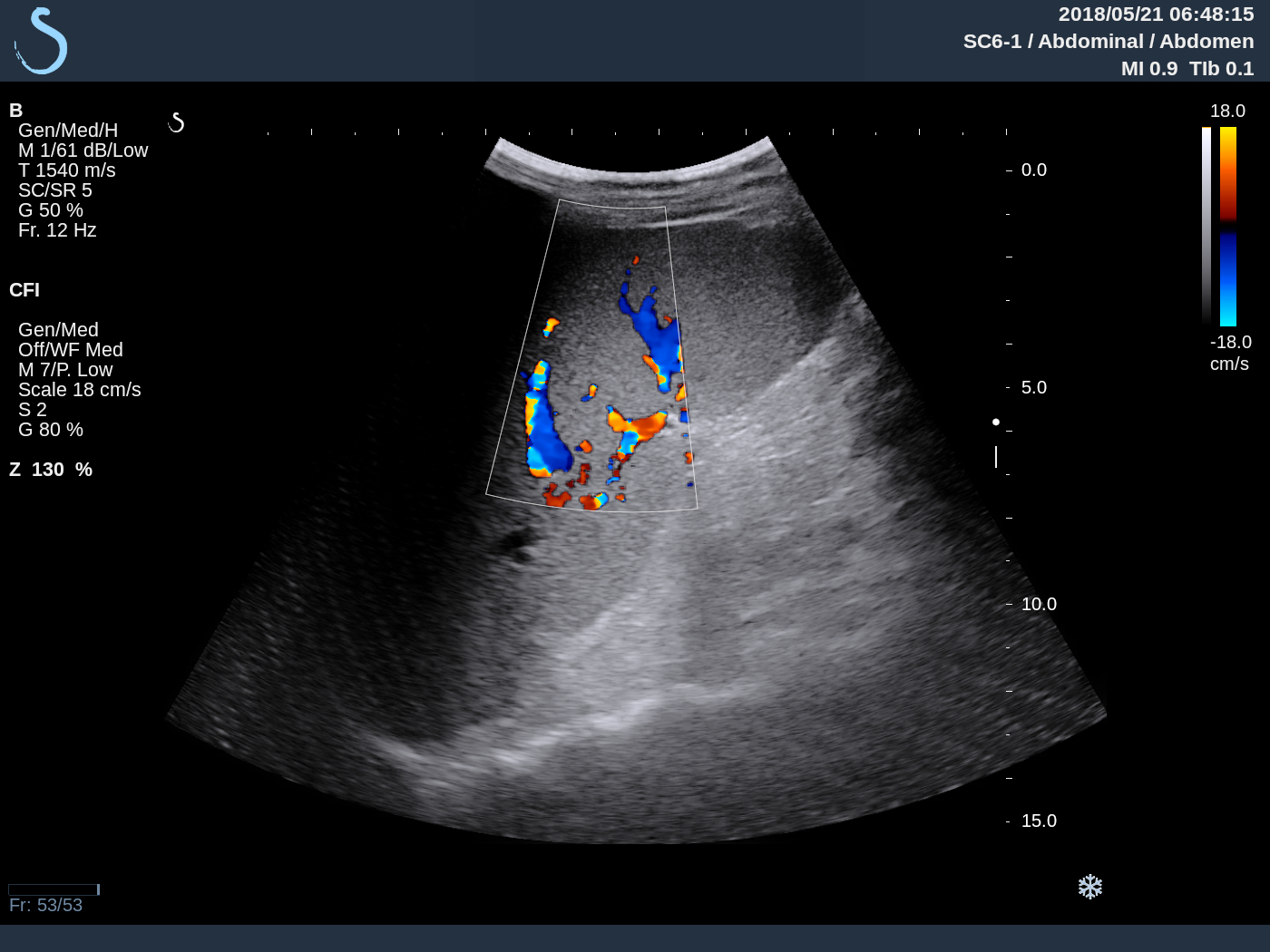
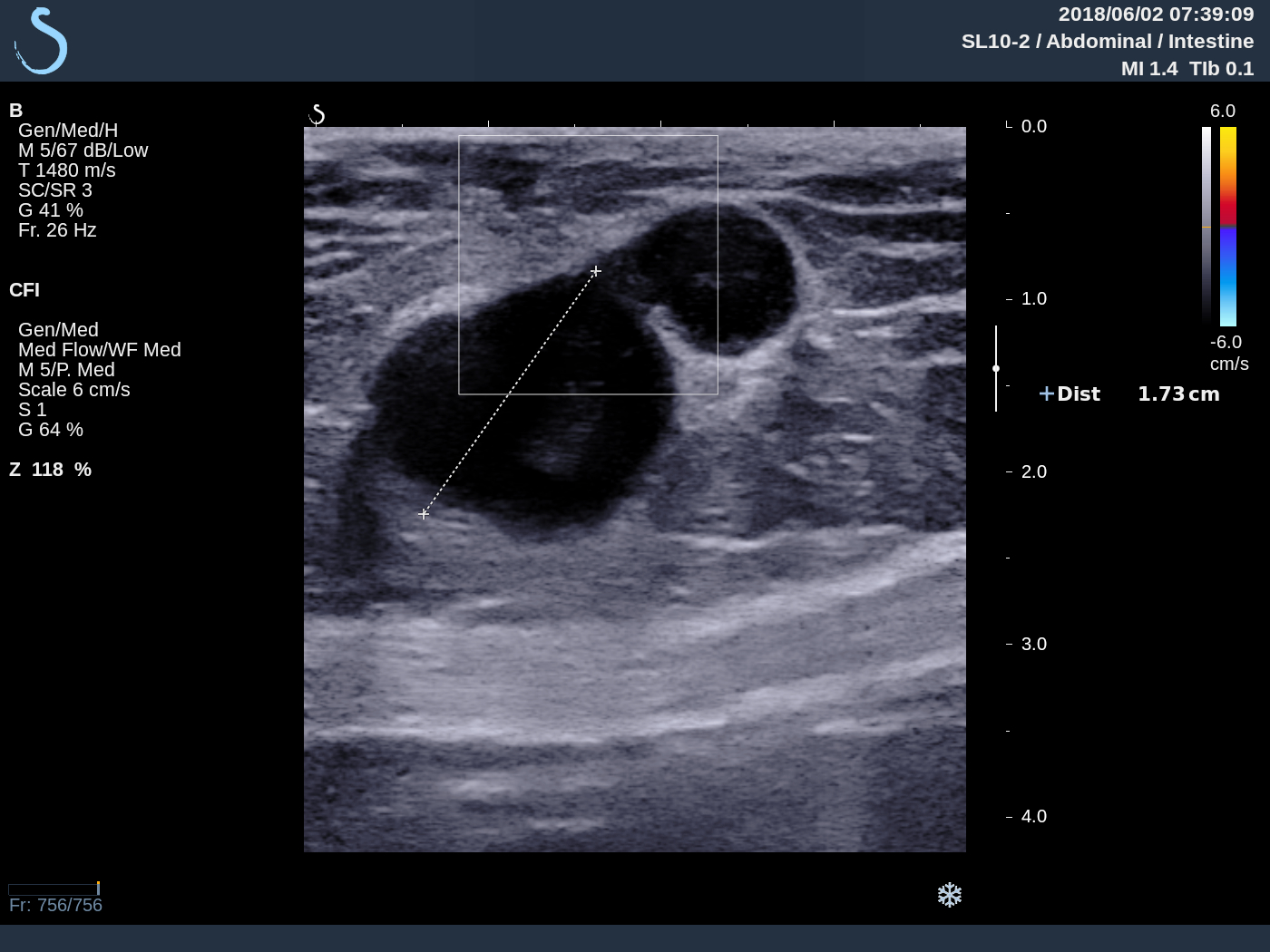
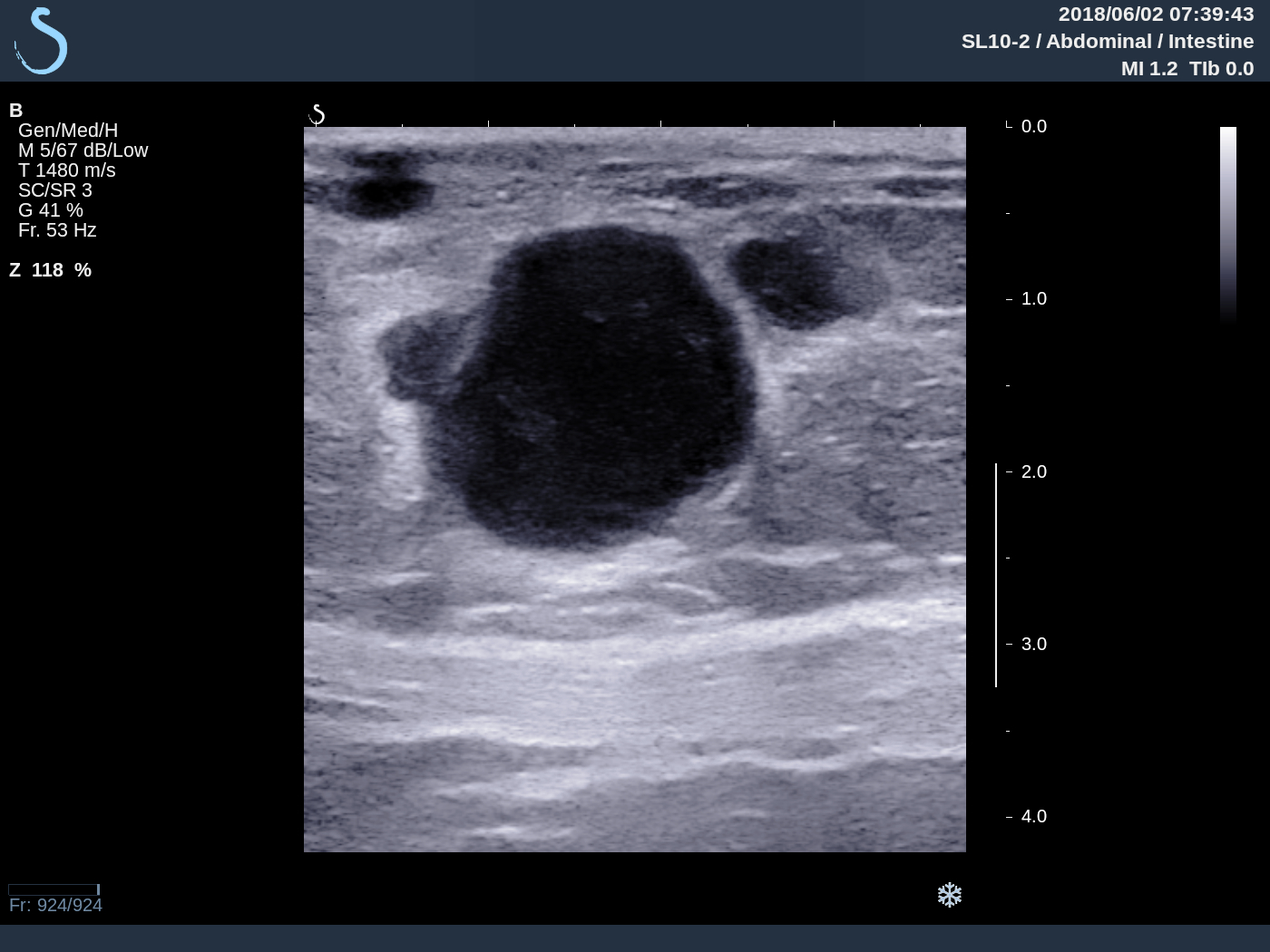
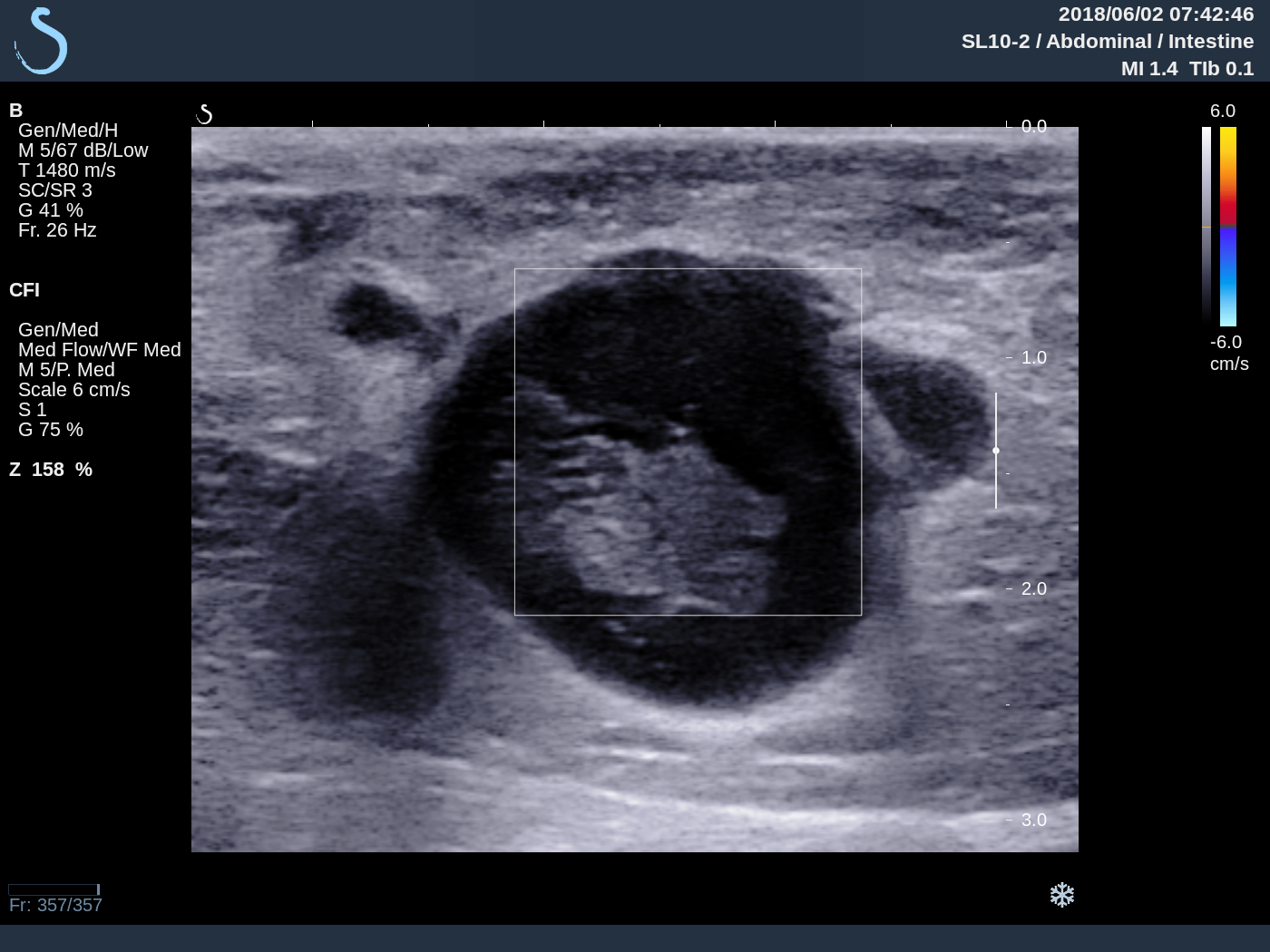
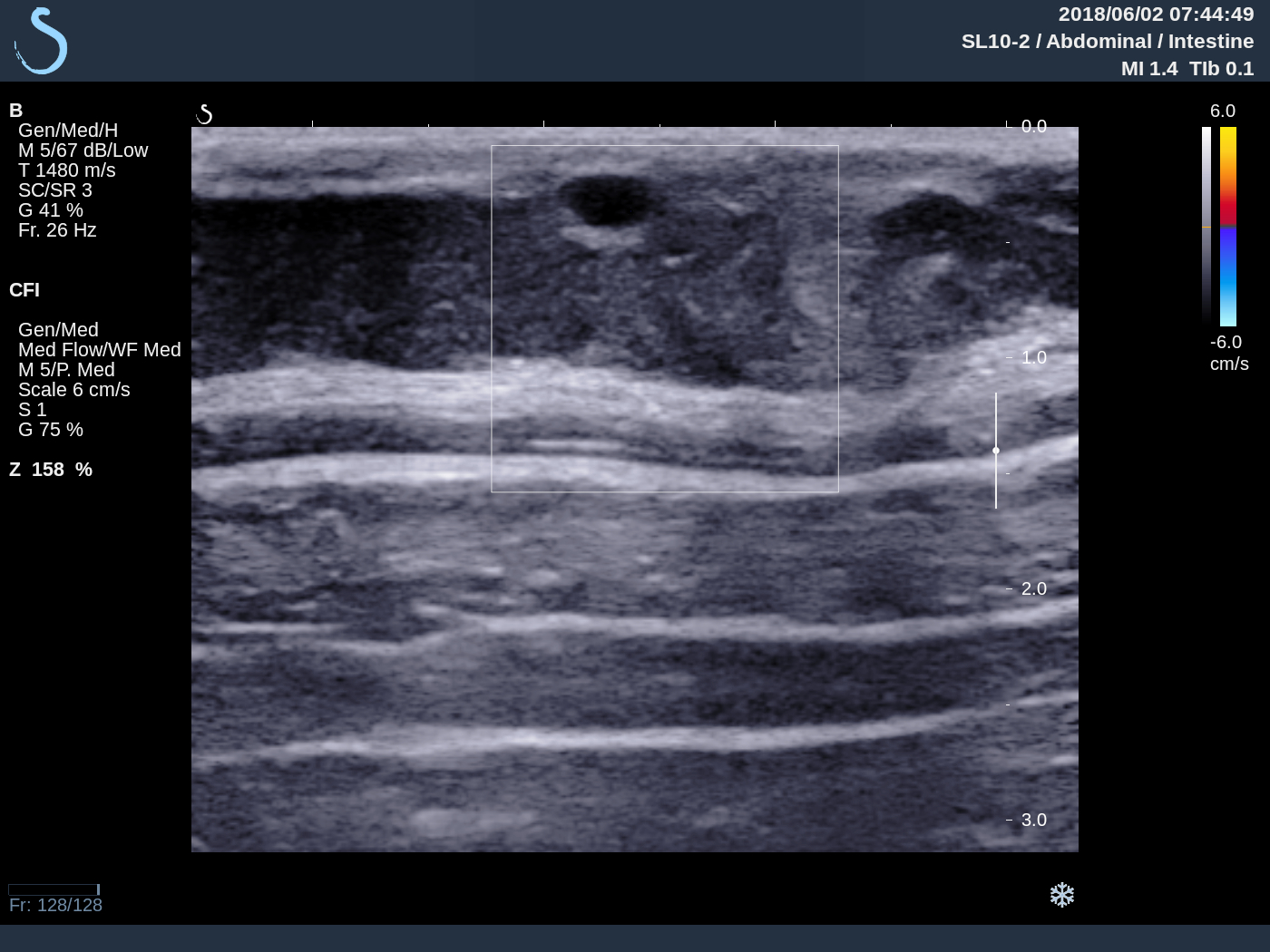
Ultrasound of abdominal wall and the leg skin lesions detected many small hypoechoic nodules with size 1-3 cm, well bordered no vascular inside lesion. Elastoscan is cystic lesion (US 1, US 2, US 3, US 4, US 5, US 6 skin).


Ultrasound guided puncture showed pus and operation removed this mass looked like caseum.
Pus analysis no bacteria. ADA very high 691.1. But PCR of BK negative.


BIOPSY OF SKIN LESION REPORTED TUBERCULOSIS.
SUMMARY: IT IS CASE OF MULTIPLE SKIN LESIONS AND SUBCUTANEOUS ABCESS DUE TO TUBERCULOSIS.