Female patient 16 yo
with epigatric pain.
Blood test= HP positive.
Ultrasound
detected left liver tumor.
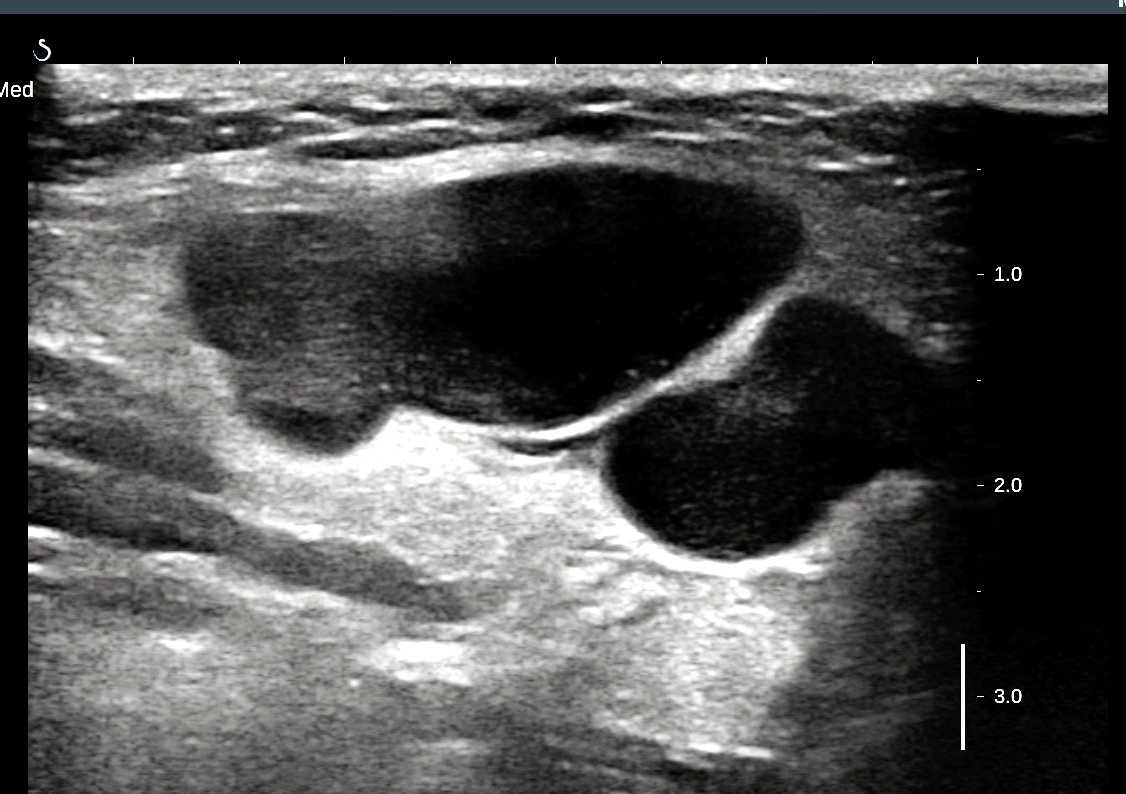
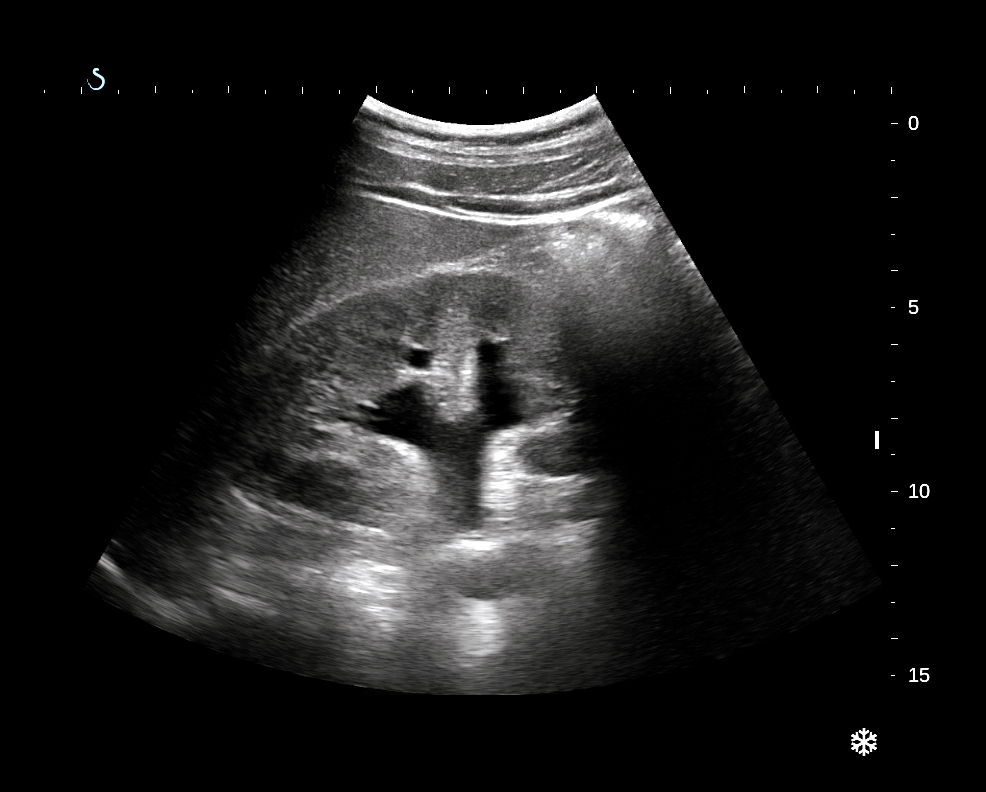
US 1 =
longitudinal scanning of left lobe of liver: solid tumor , size
of 10 cm with central necrosis.

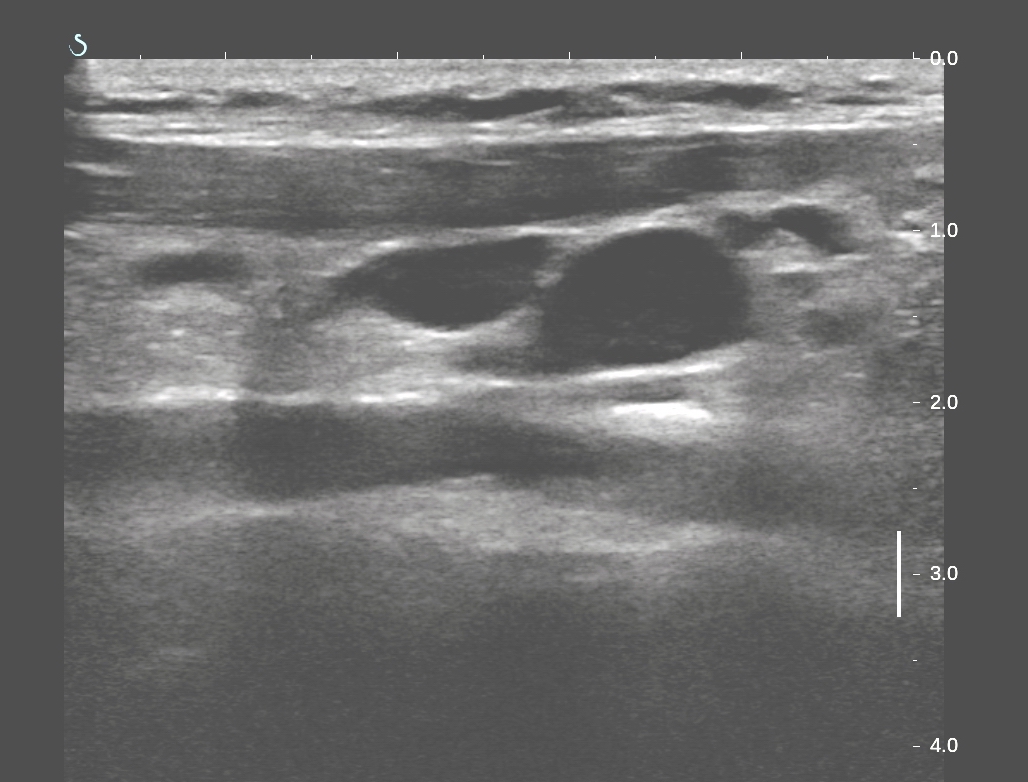
US 2 = subcostal
scanning : tumor covers left liver lobe.

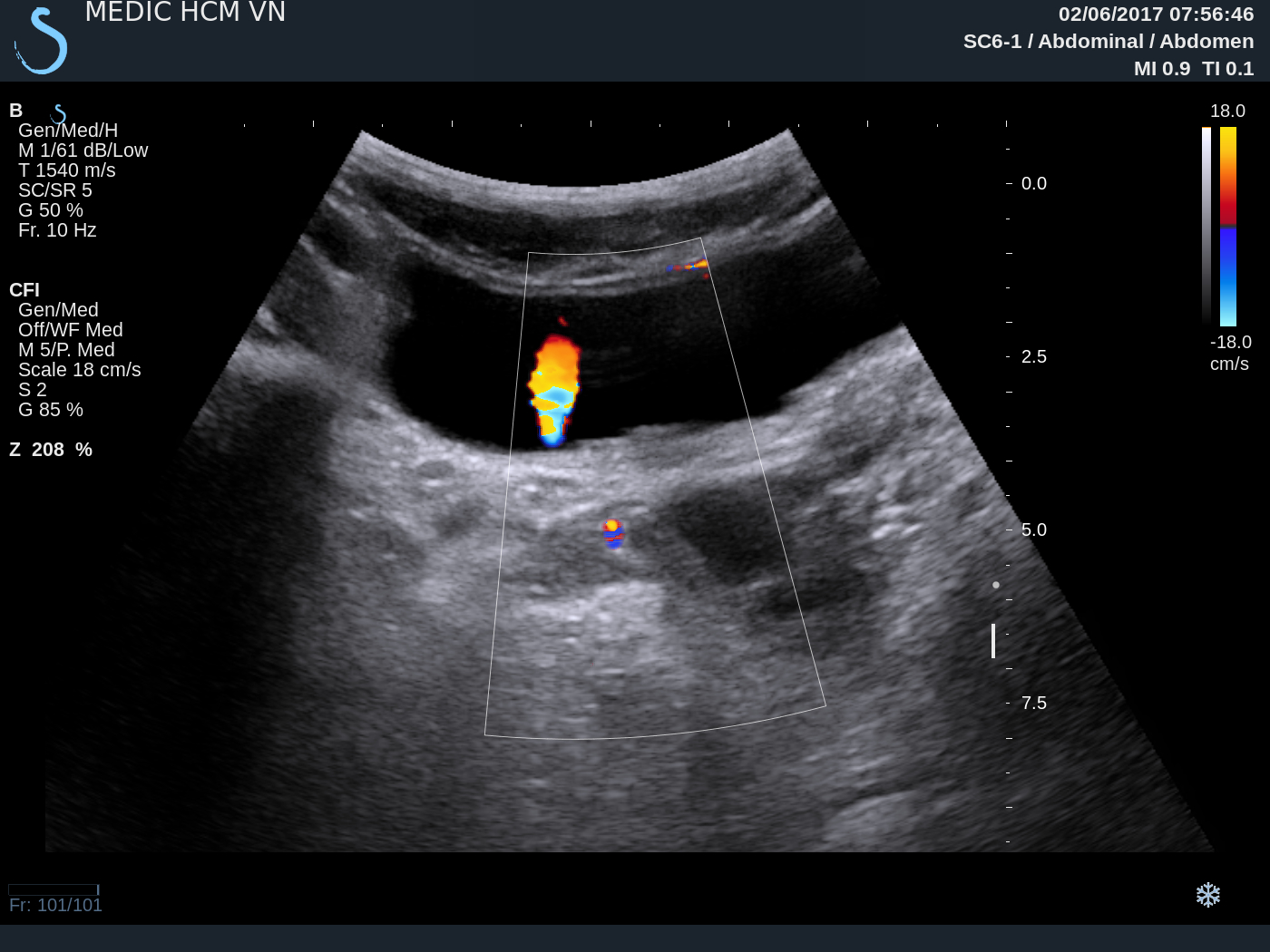
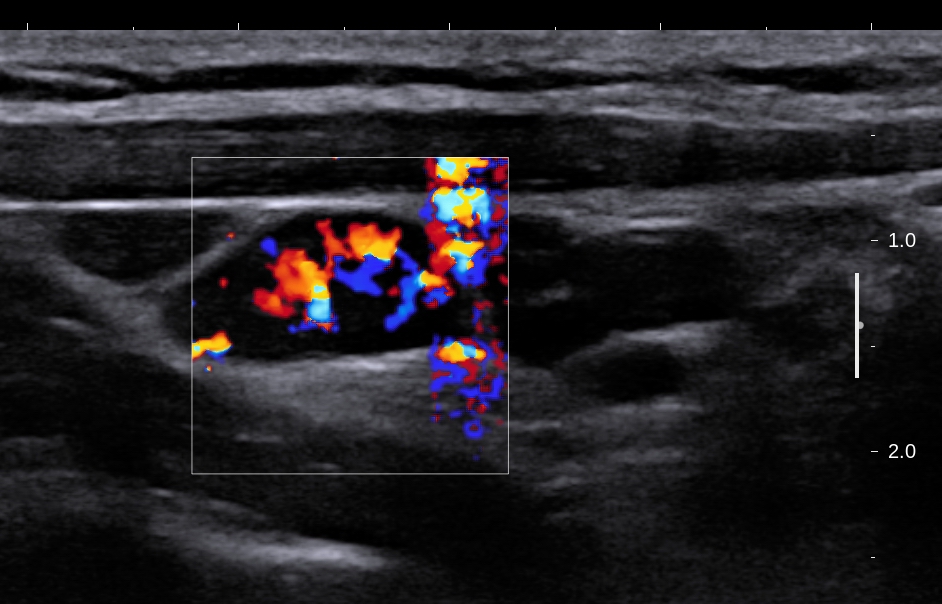
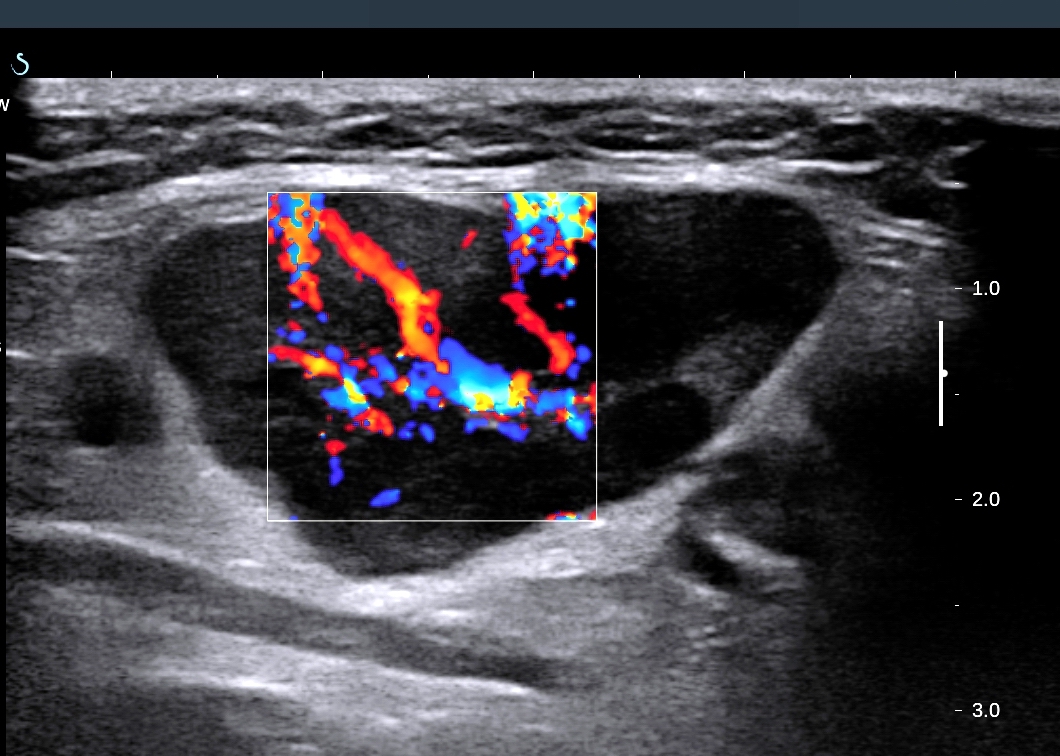
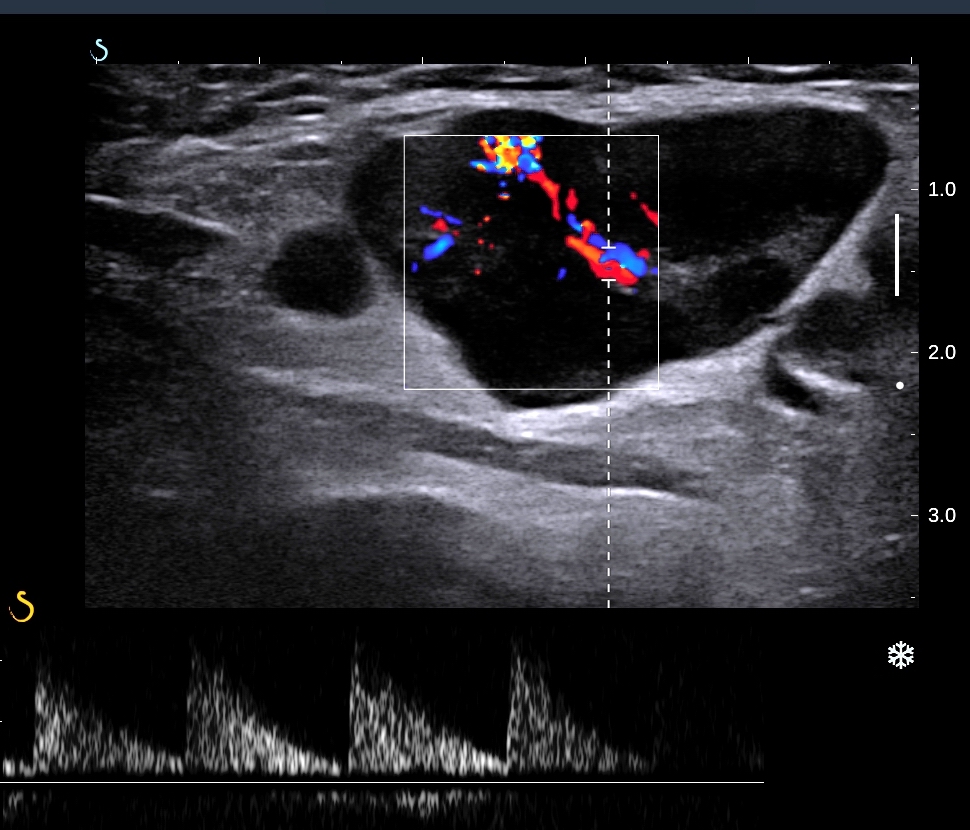
US 3 = color Doppler
: vascular supplying of this
tumor.

US 4 = elastoscanning
of this tumor = 10,5-15 kPa.

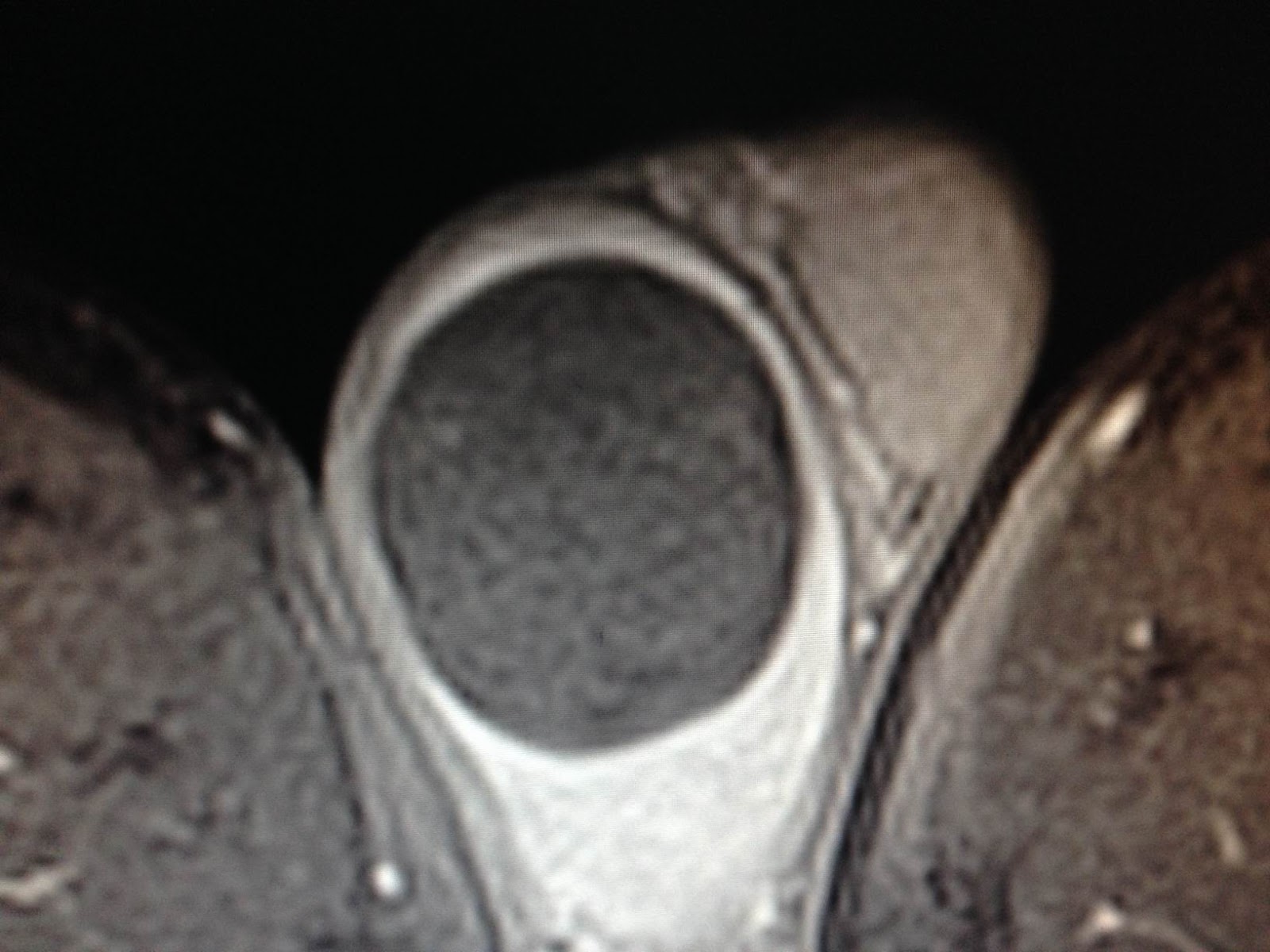
MSCT with CE: CT 1, CT 2 = artery and vein phases, CT 3 = frontal
view of this tumor from left liver.



Blood tests= no
infested HBV, HCV, Wako tests 3 negative.

OPERATION WAS DONE FOR RESECTION OF THE TUMOR (SEE MACRO).


Macroscopic is FNH.

Liver tumor FNH or HCC