Woman 43 yo with sorethroat and cough, sputum
bleeding.
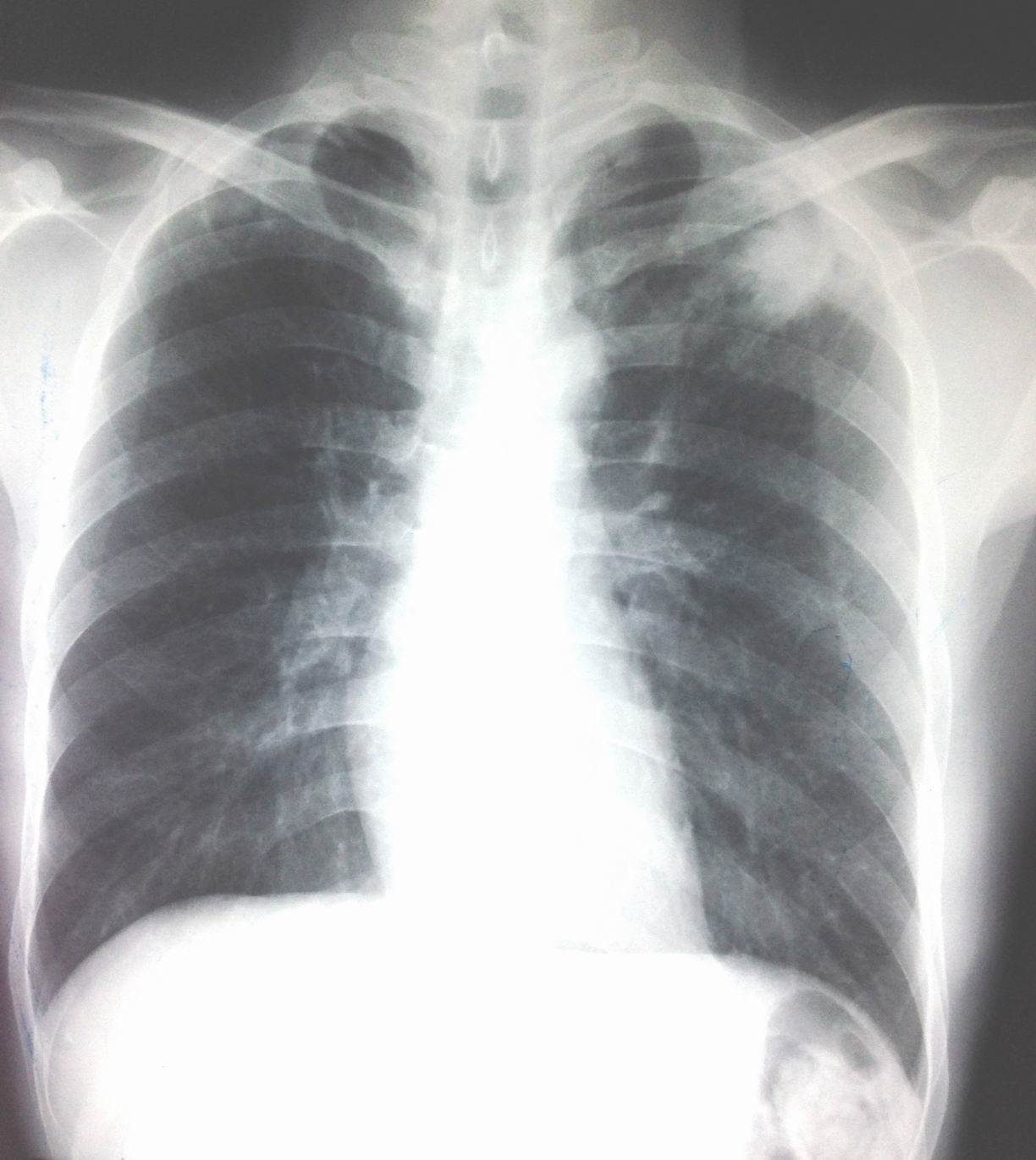
Chest X-Rays for screening: no chest lesion ( see foto chest
X-Rays).

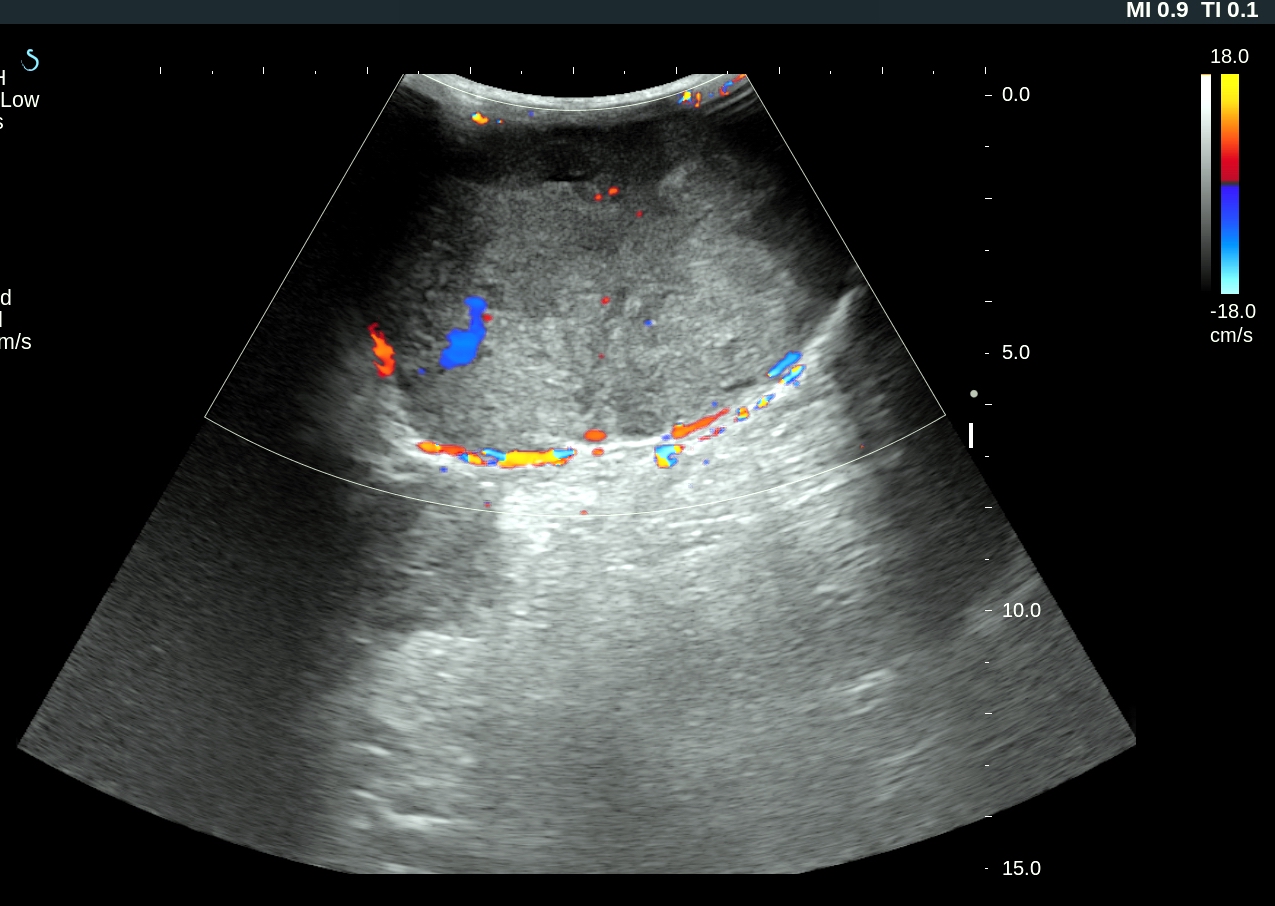
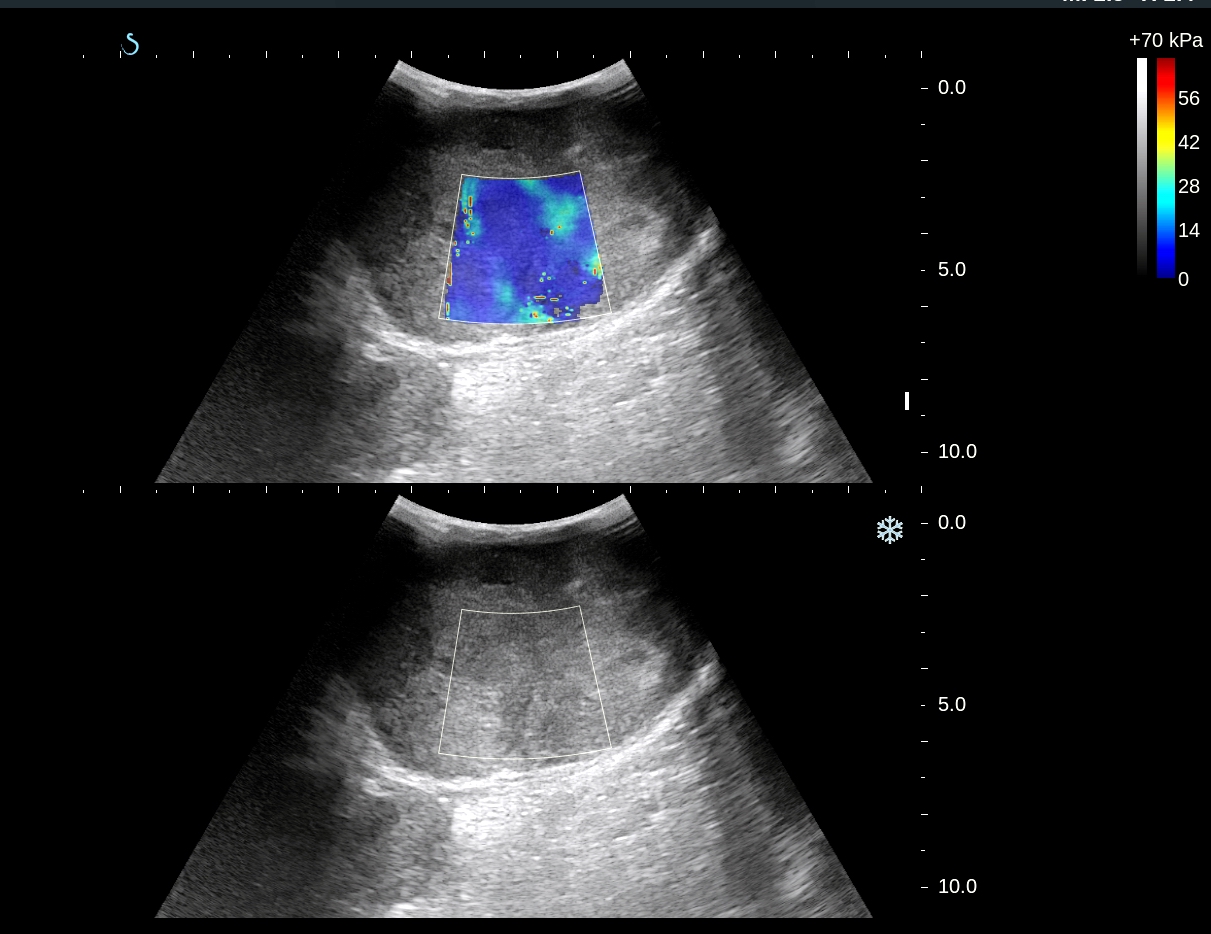
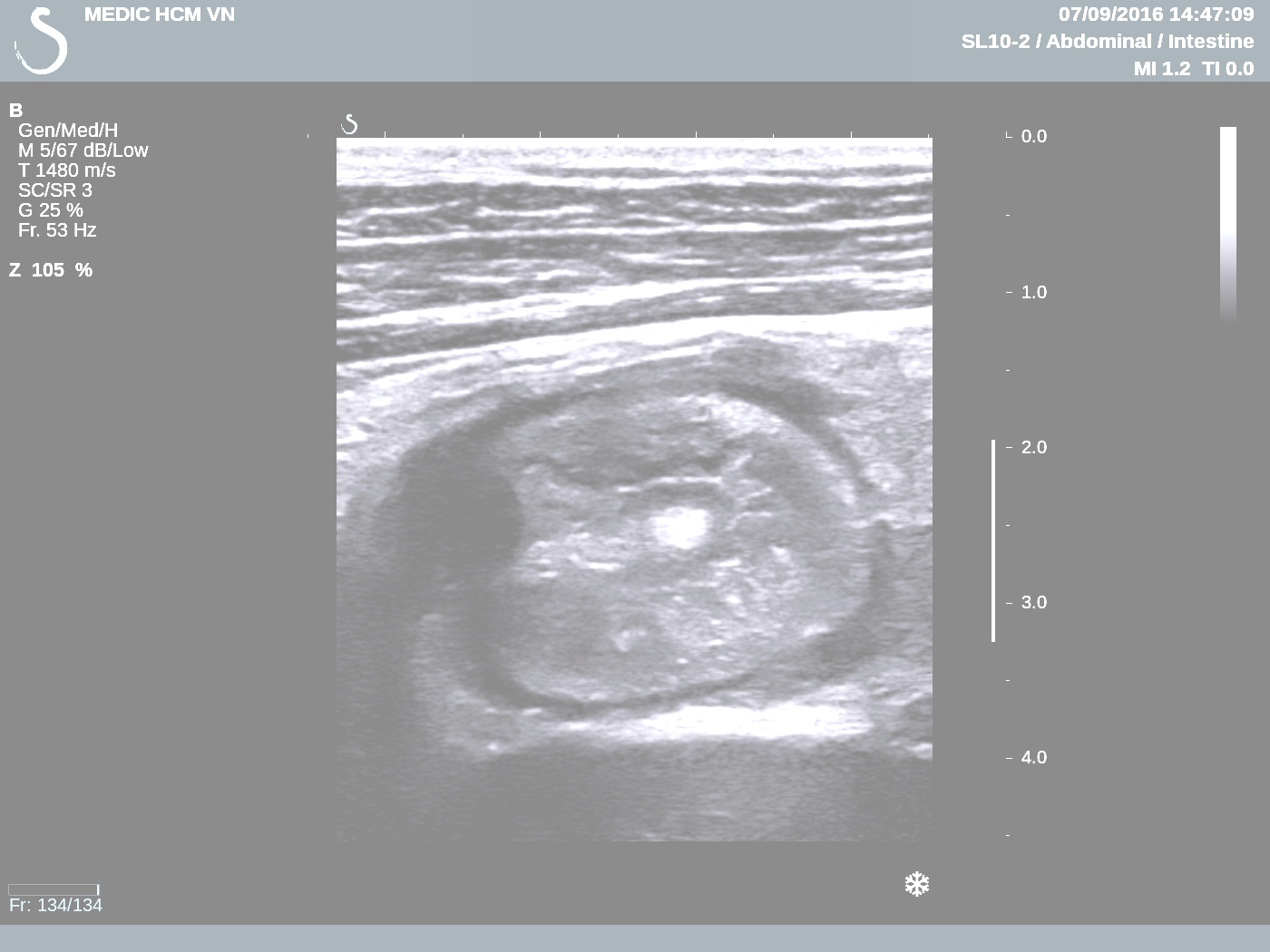
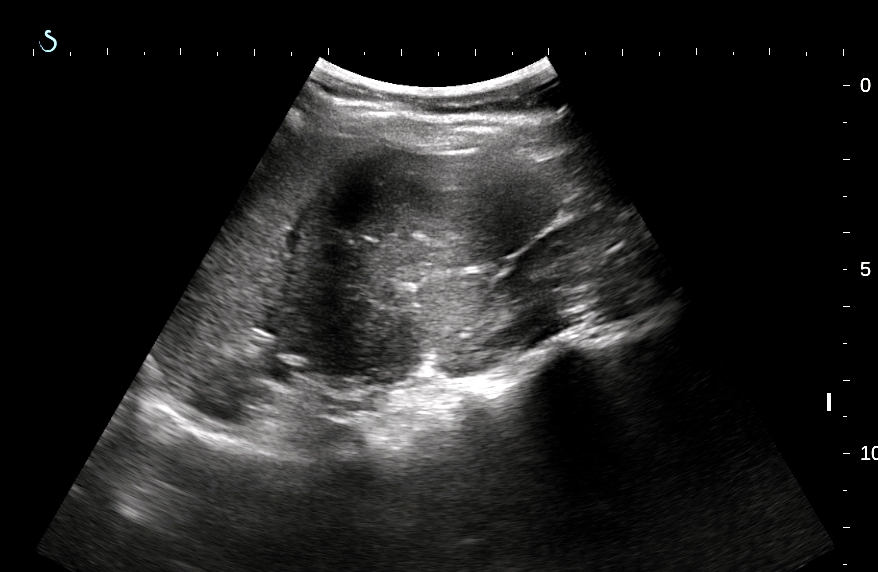
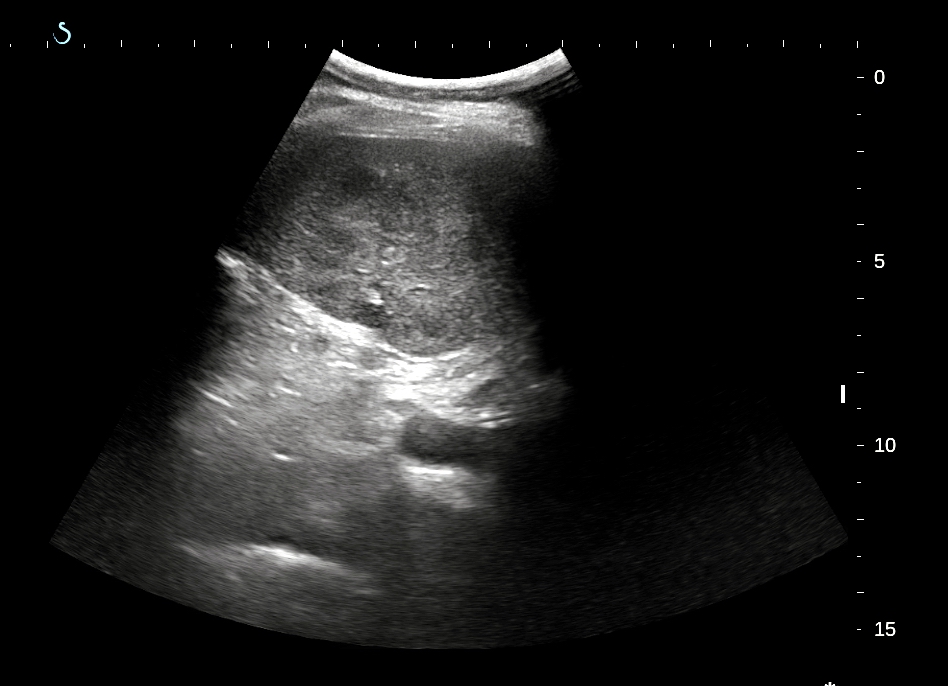
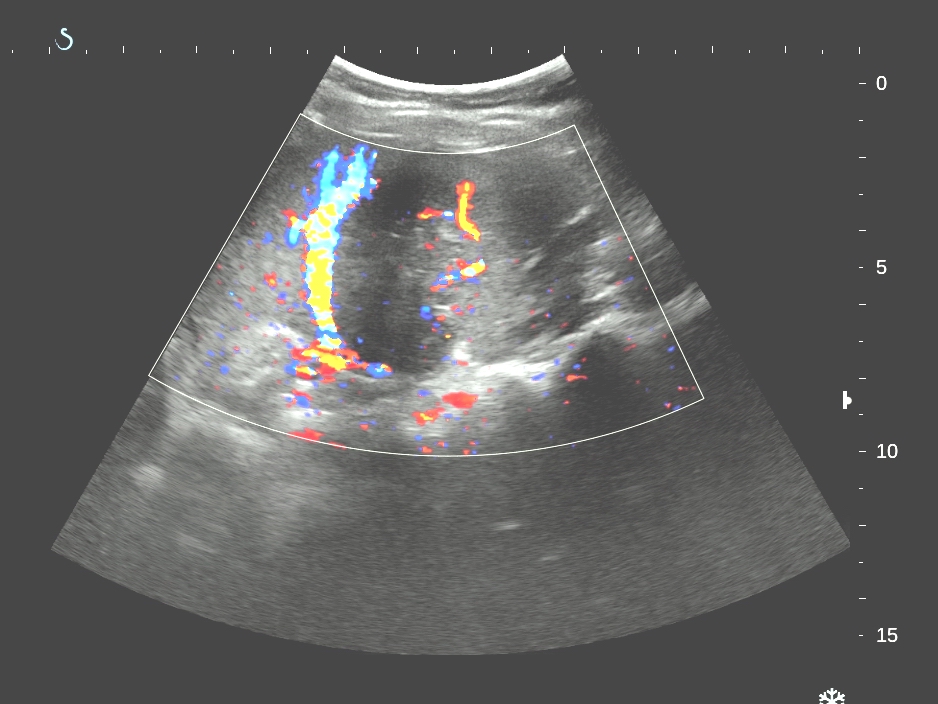
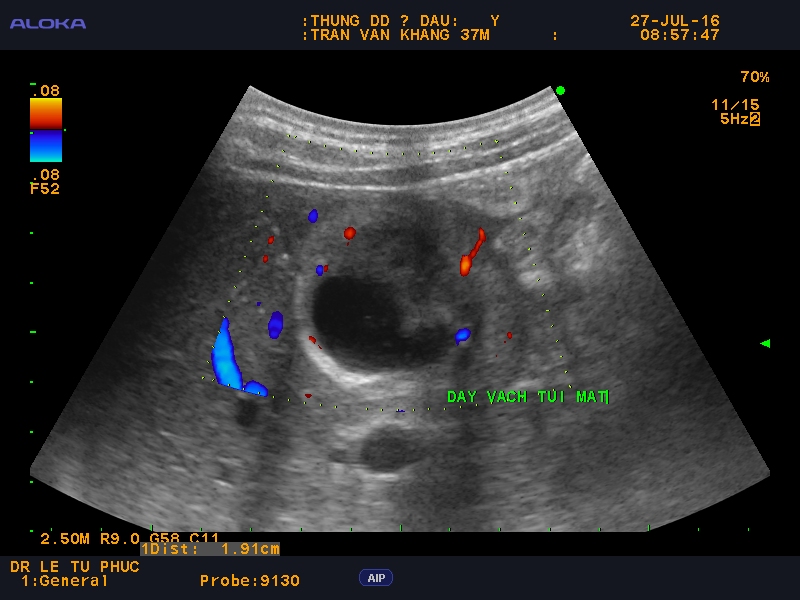
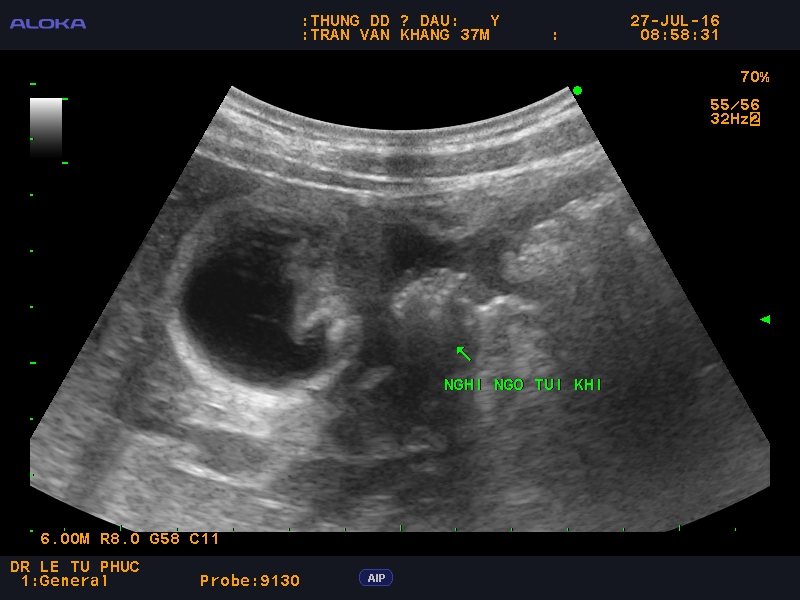
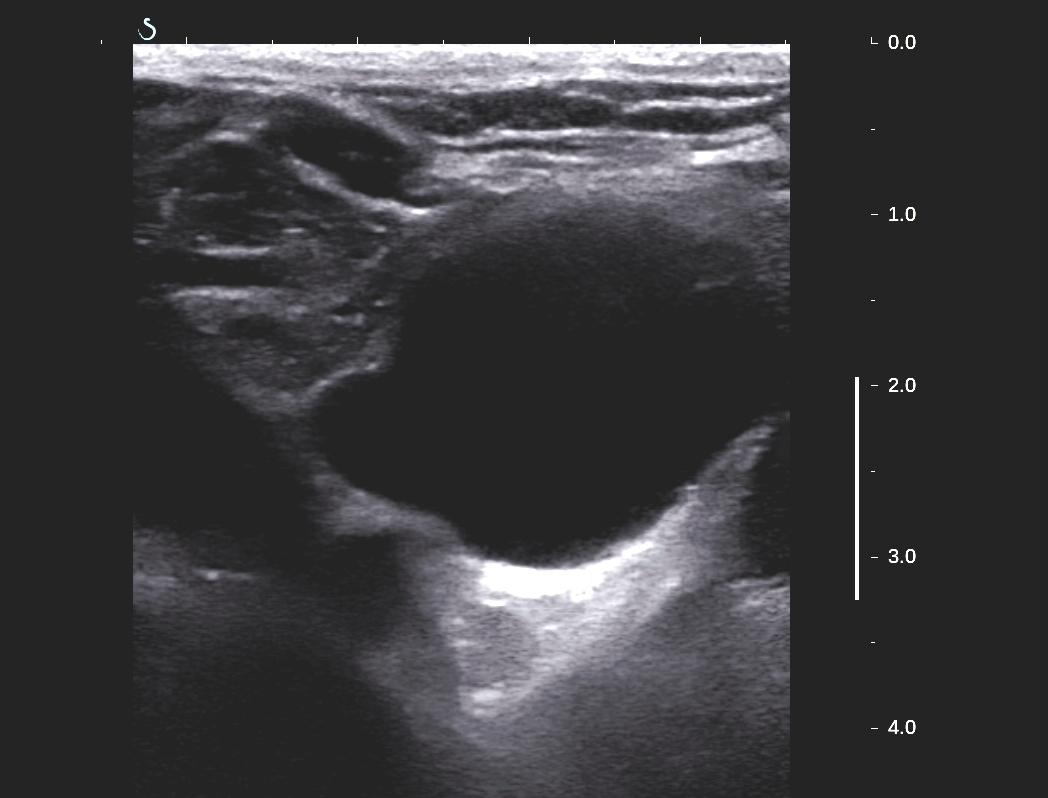
Ultrasound of the neck: normal thyroid but detected
a cyst at lower pole of thyroid gland, size of 5-6 cm, monocystic
prolonged to retrosternum.
US 1,US 2 ( CDI), US
3 pretrachea longitudinal scanning.


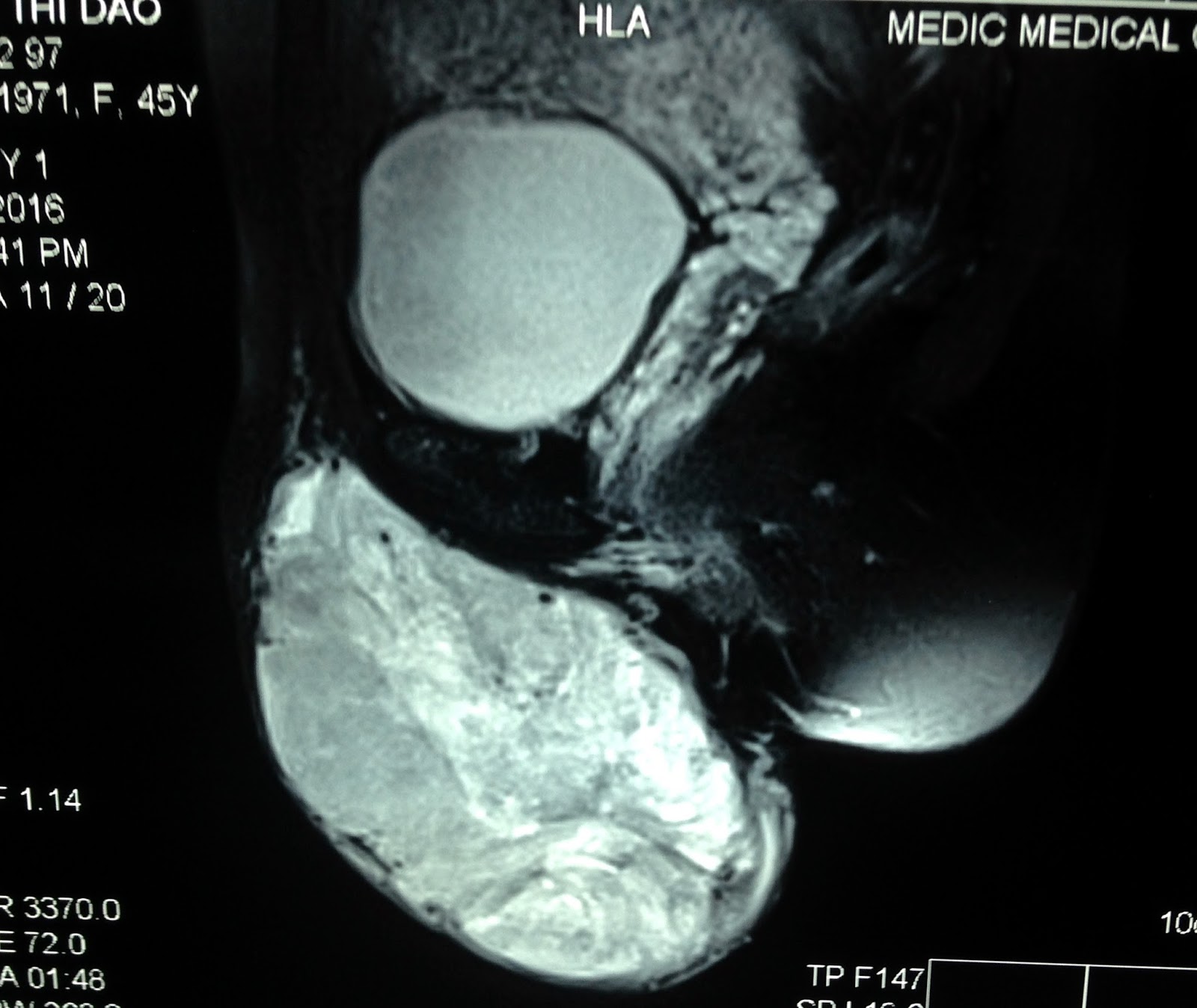
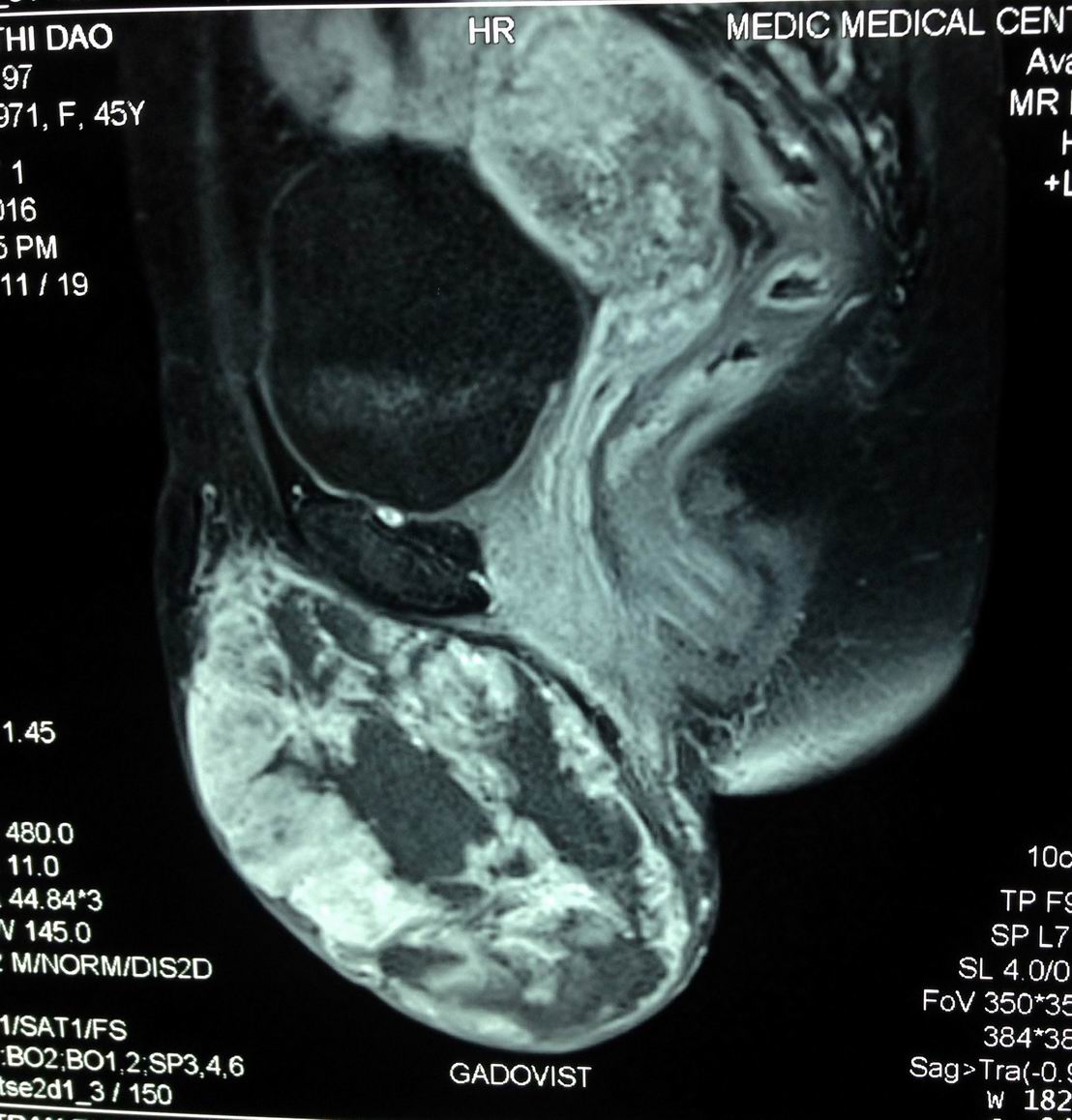
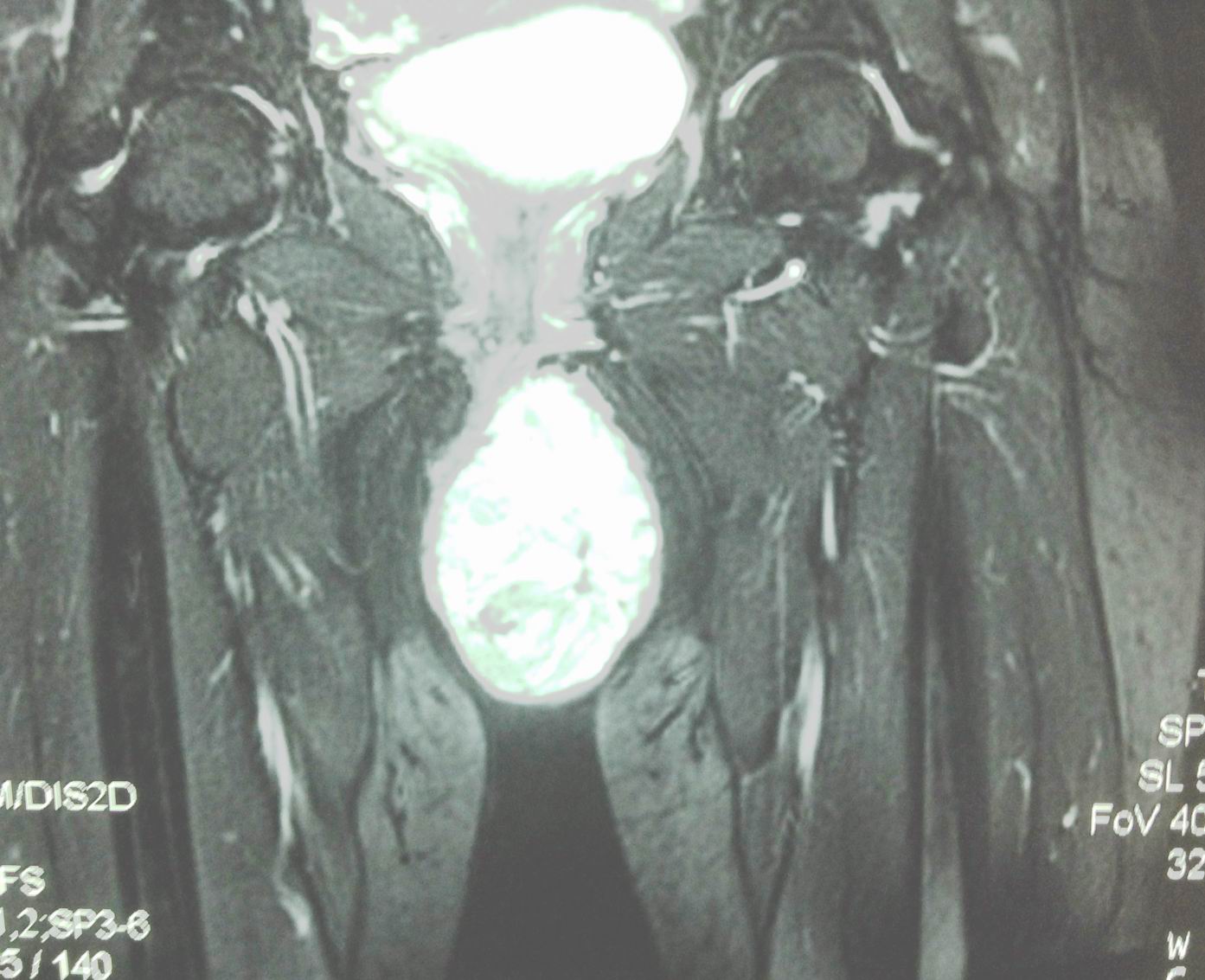
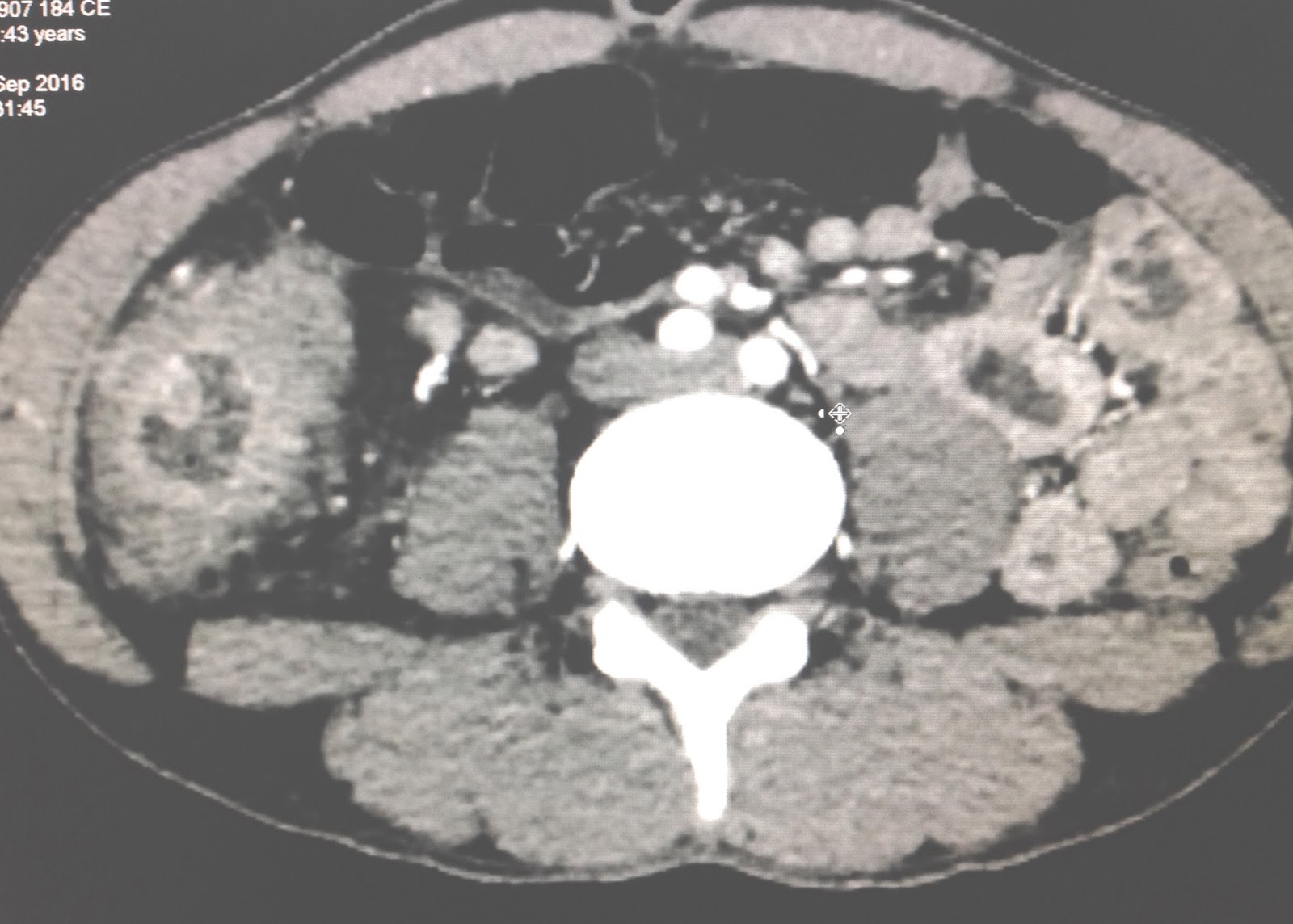
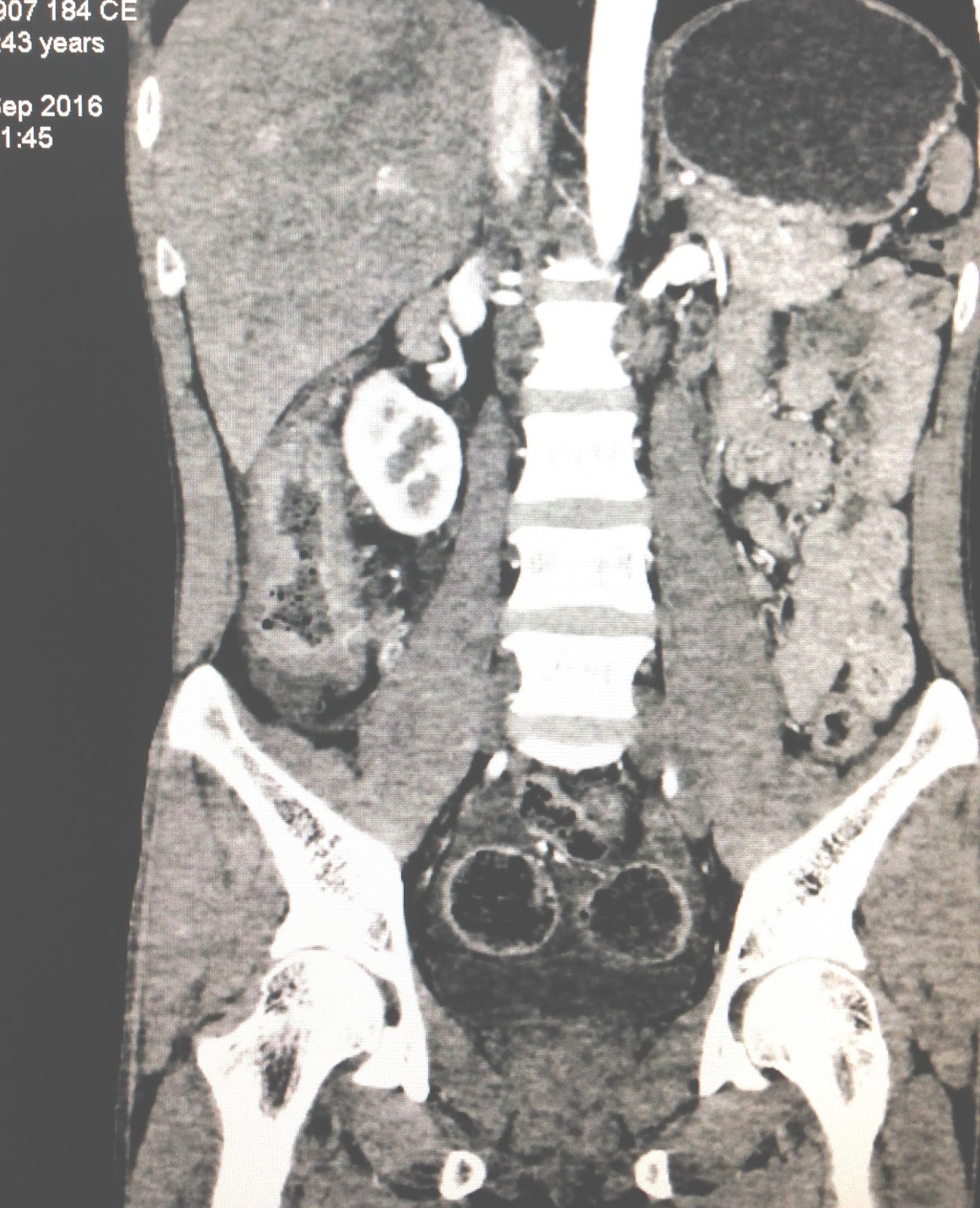
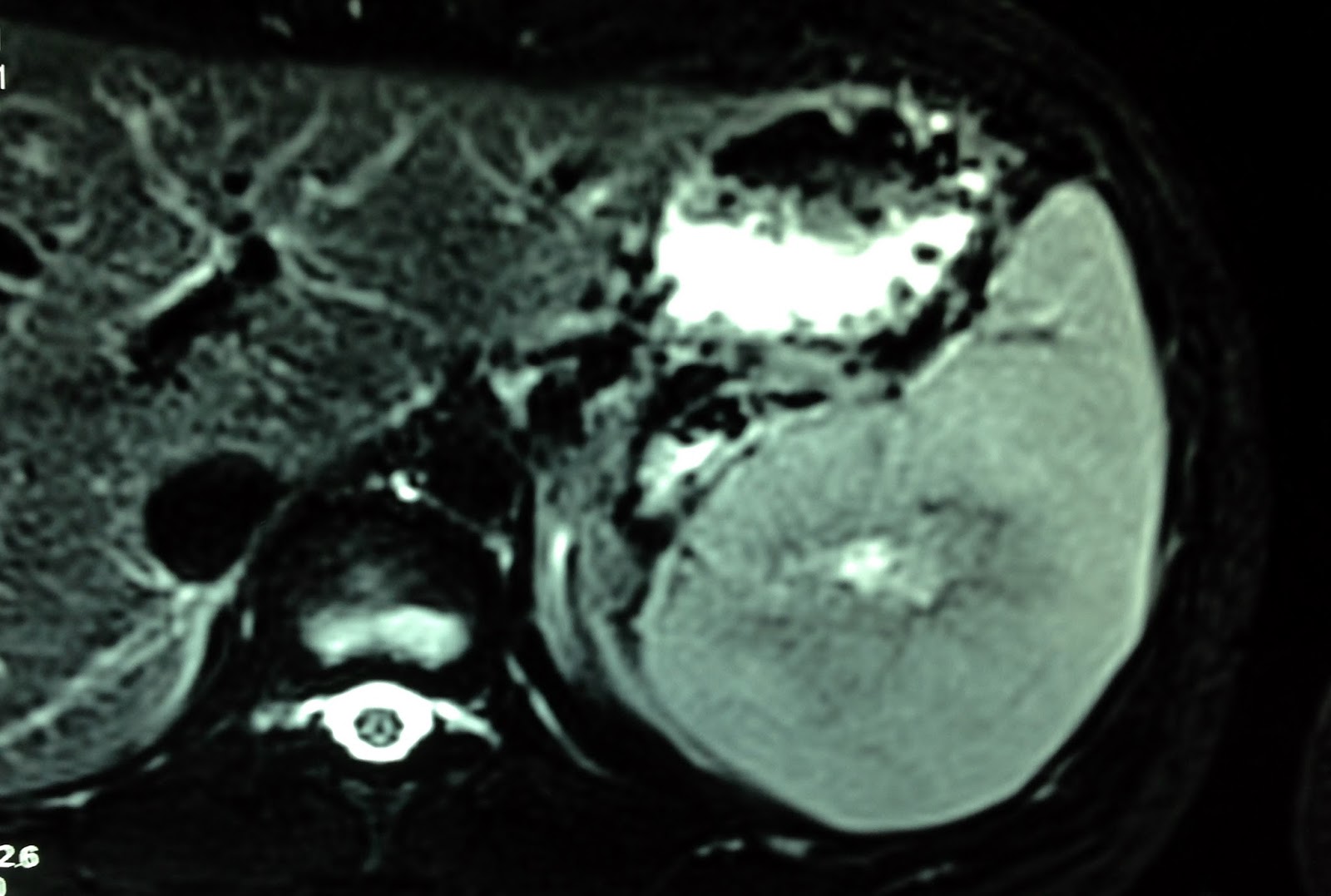
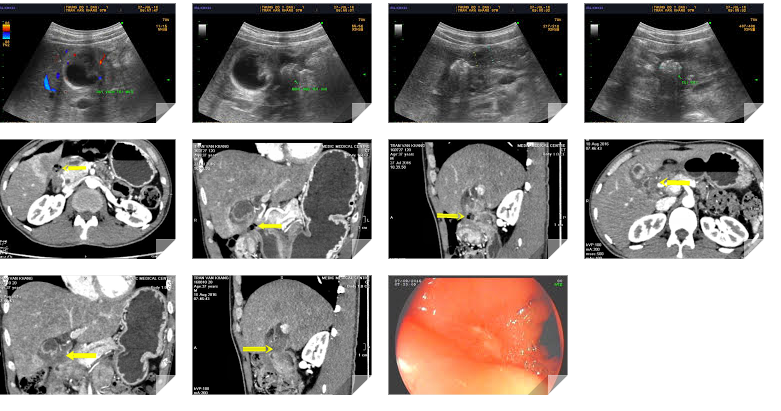
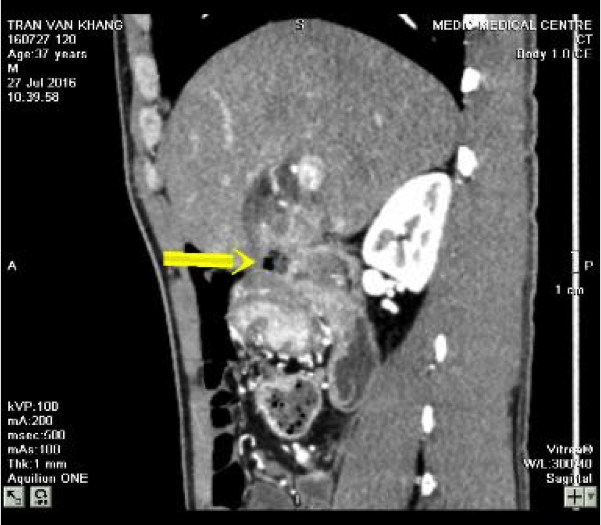
MSCT CE of the neck: CT 1=frontal
viewing, well bordered cyst, CT 2: sagittal
view..
C T 3. Cross-section= retrosternum tumor.



Ultrasound guide punction of this cyst removing 10ml clear fluid.
What do you need to study in this fluid?

The final diagnosis is non functional PARATHYROID CYST.

Reference