Woman 26 yo with no clinical symptom. Ultrasound
screening detected a spleen mass
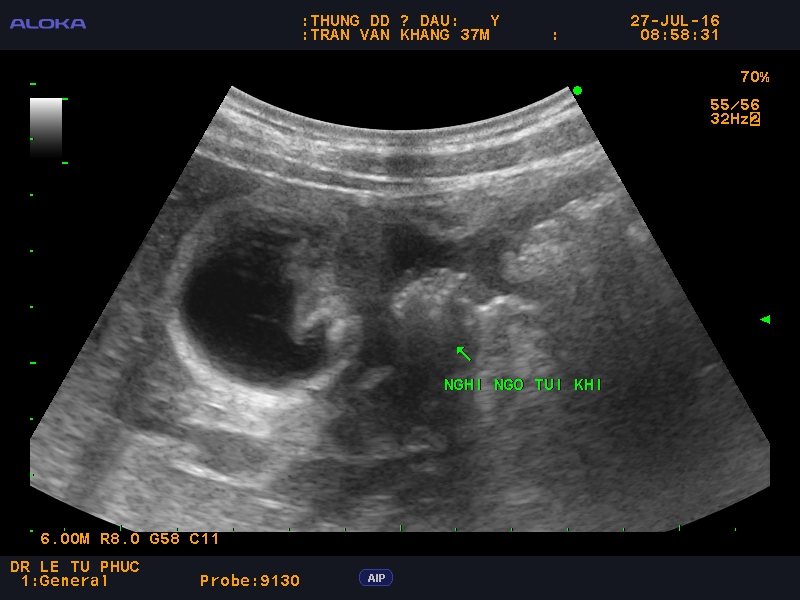
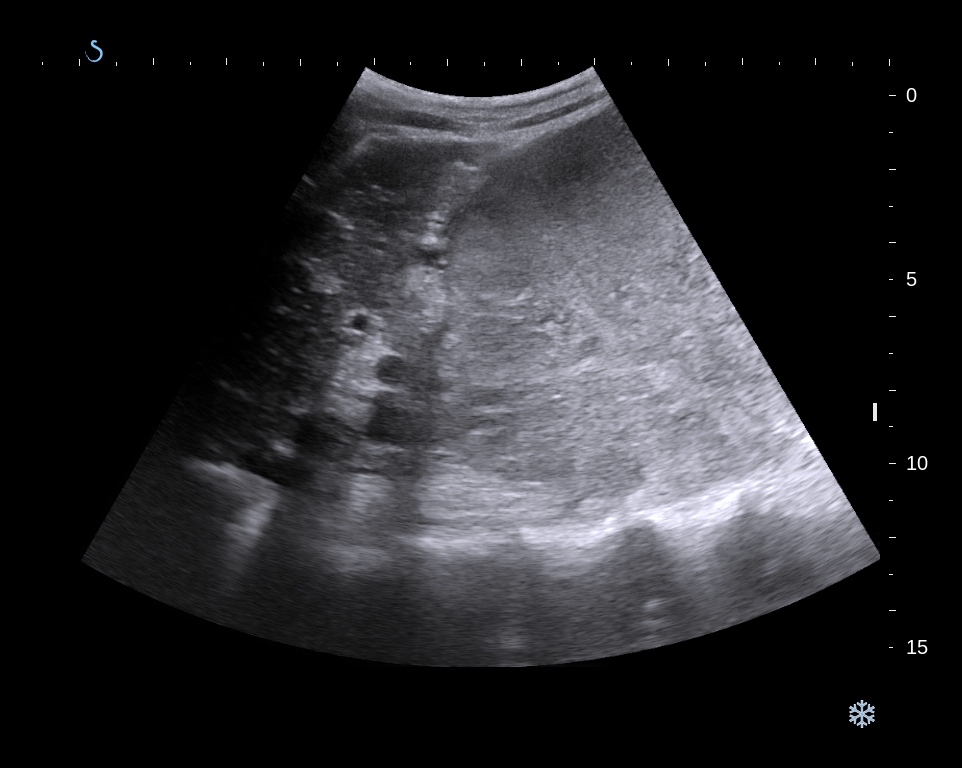
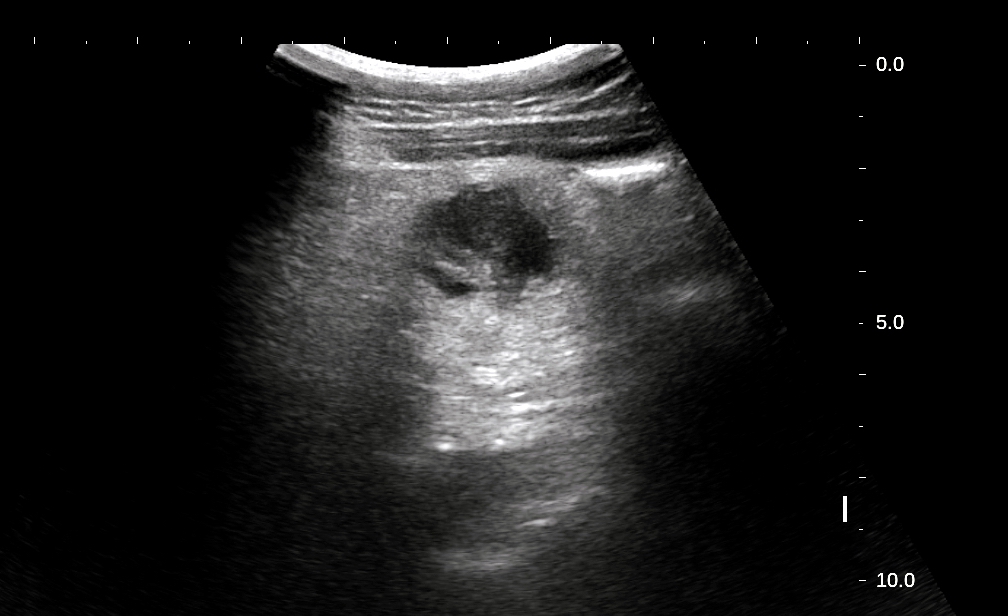
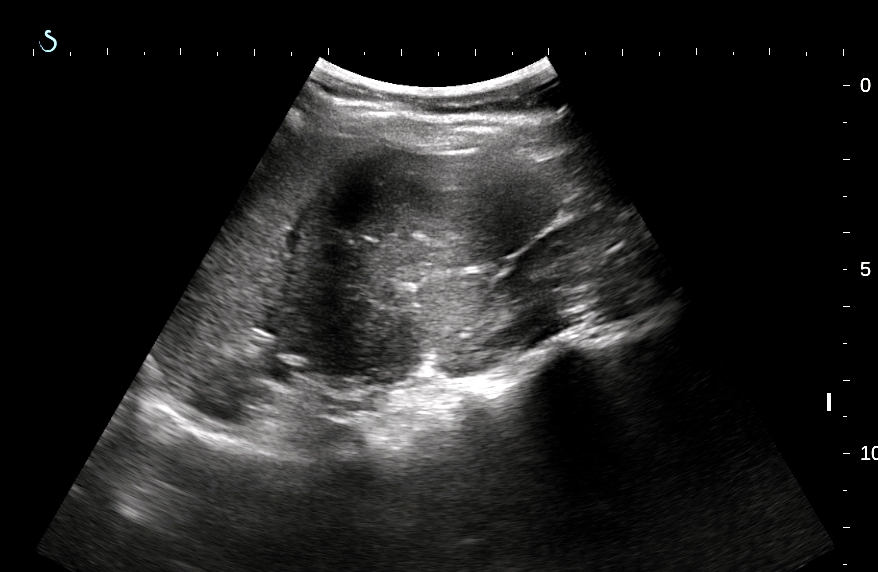
US 1= longitudinal
scan of this mass size of 6.0cm at lower pole of spleen, hypoechoic,
well bordered.
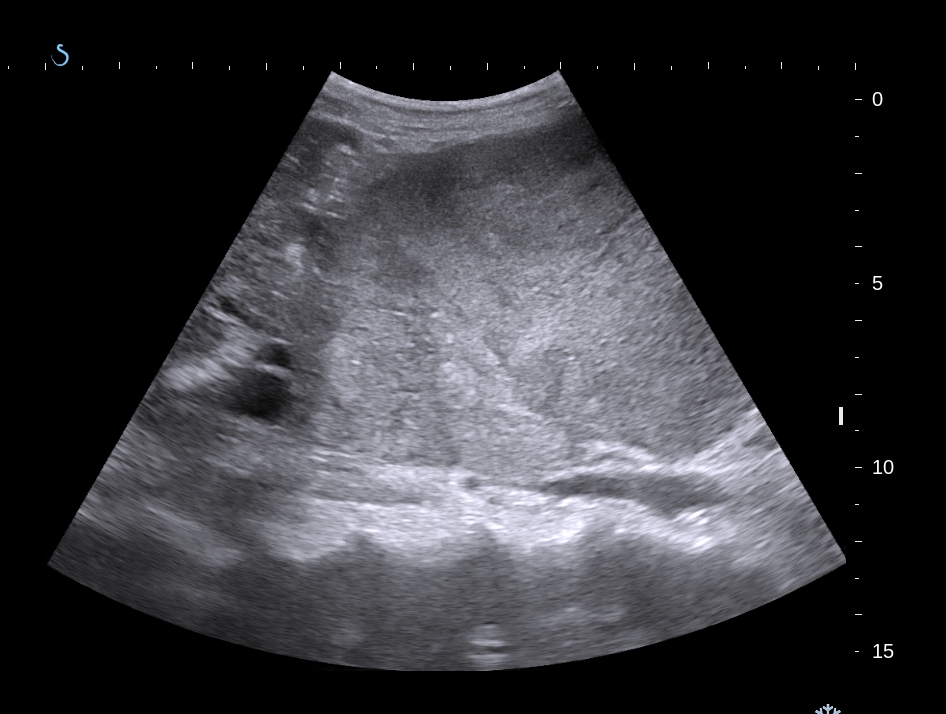
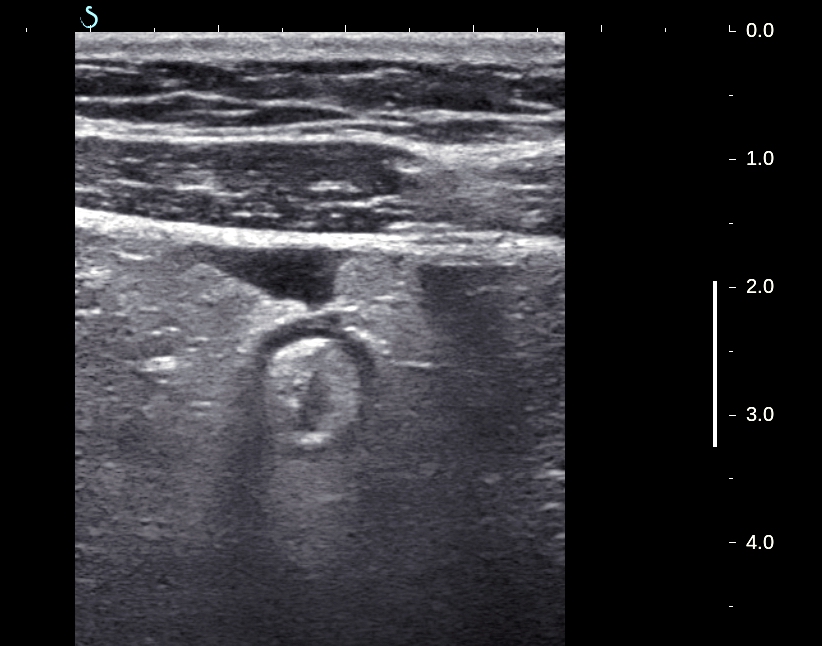
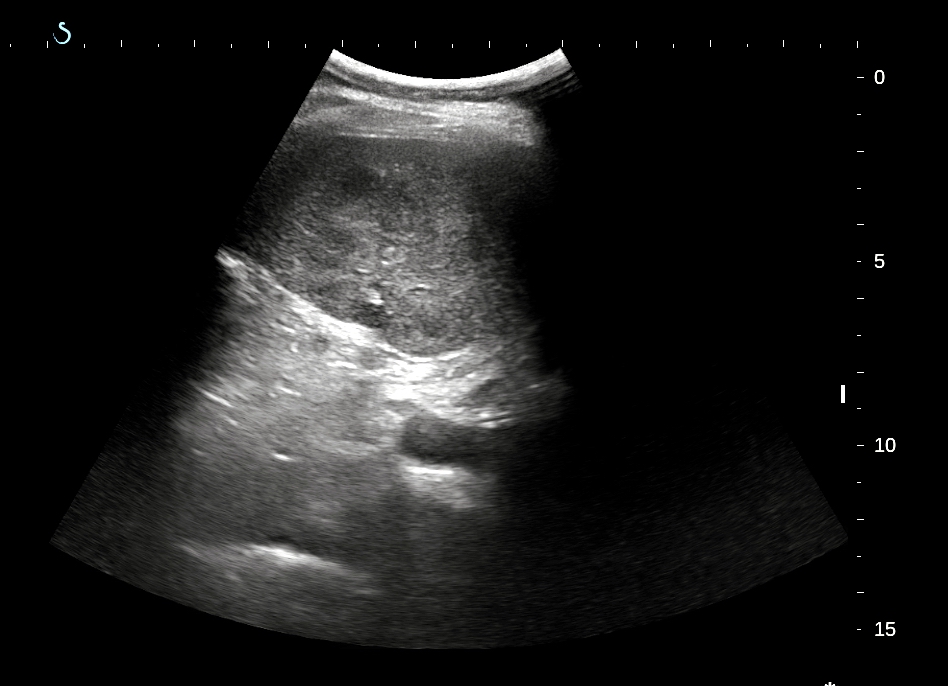
US 2=cross-sectional
view of mass.
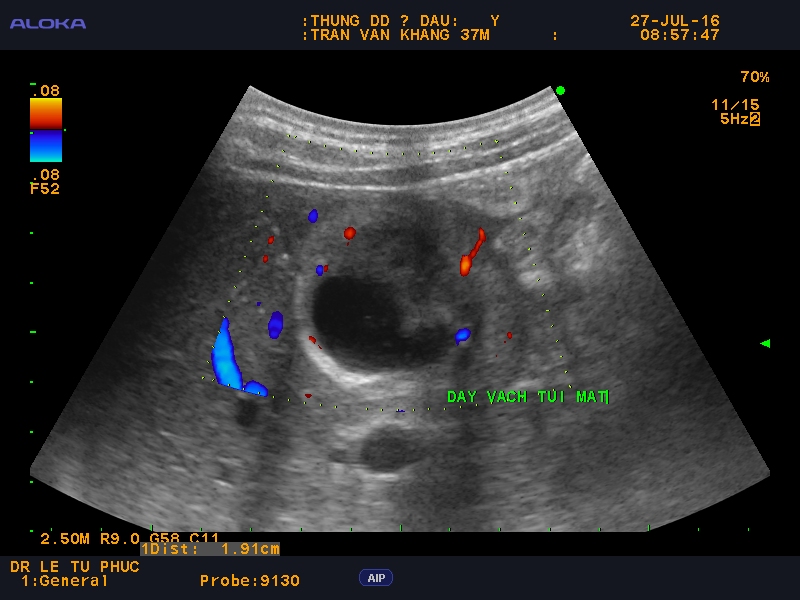
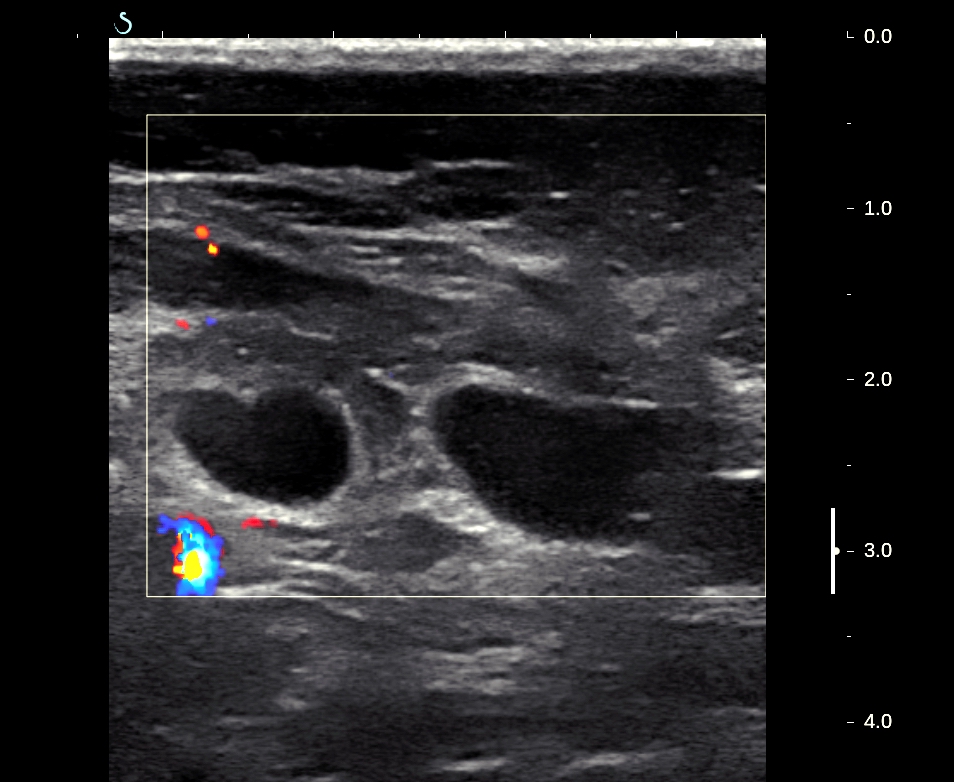
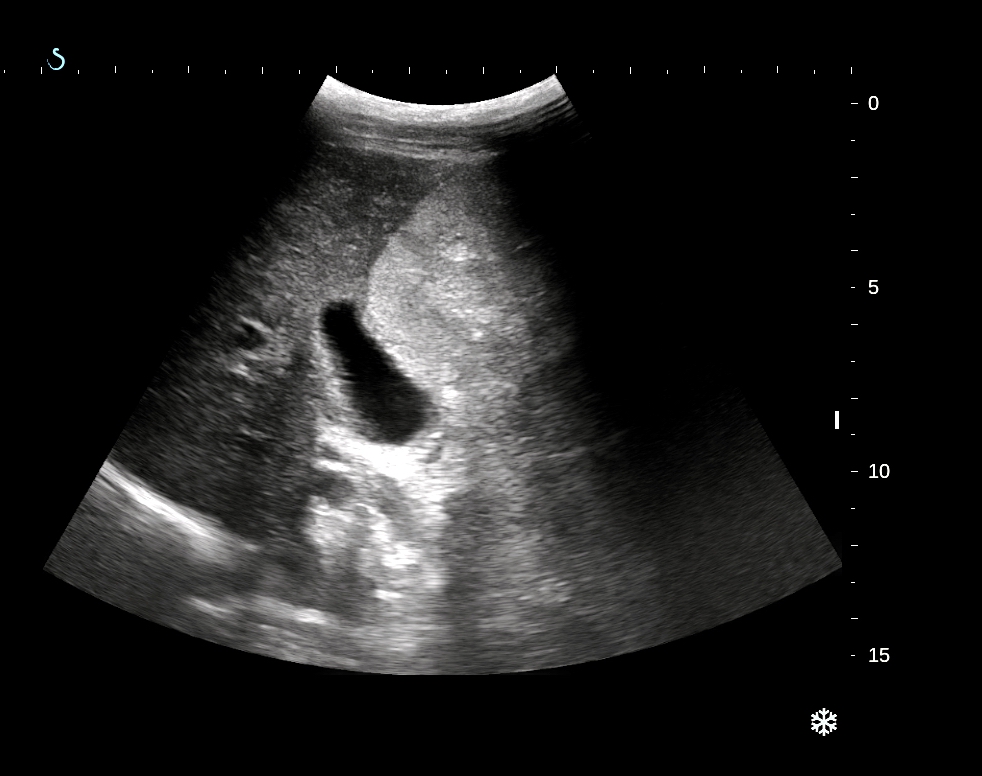
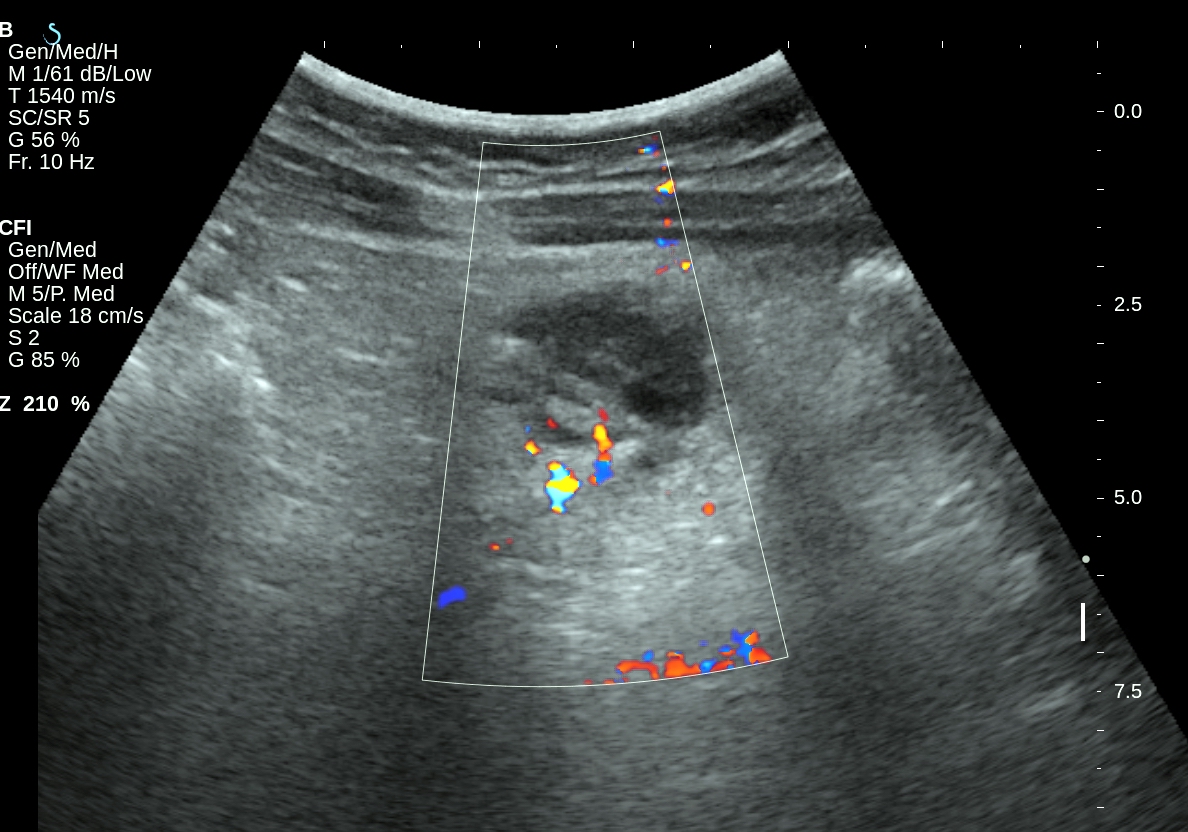
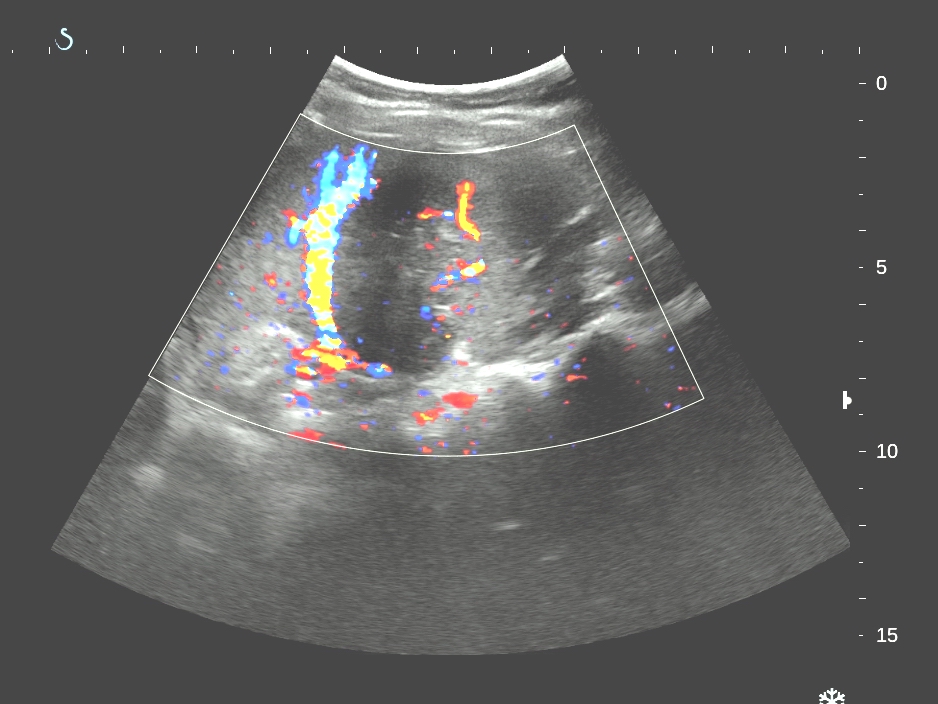
US 3=CDI of this
mass with vascular bending sign and, ( US 4) structure inside
hypervascular.

Blood tests are
normal.
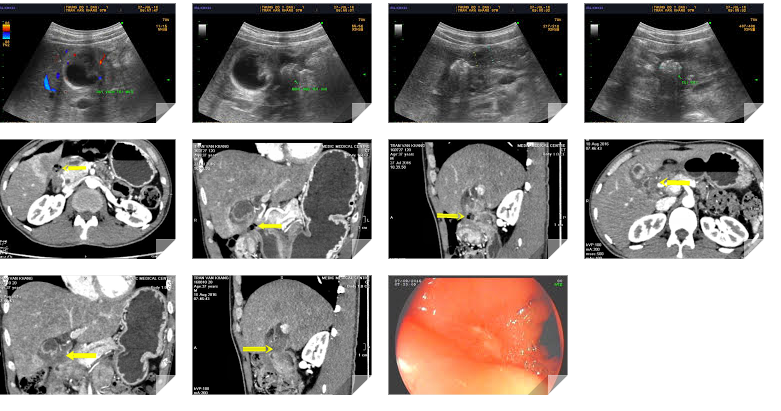
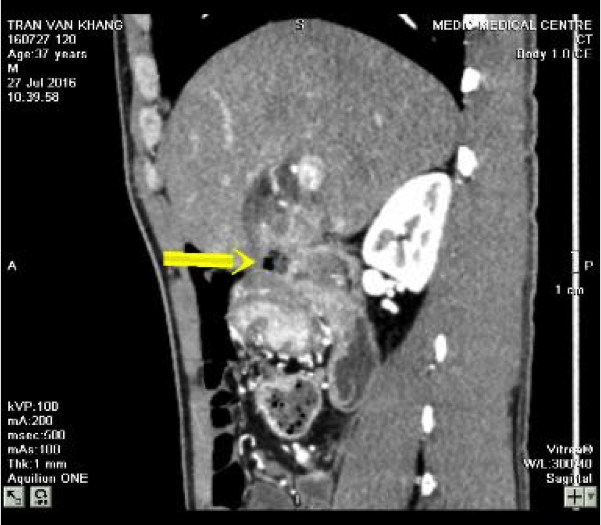
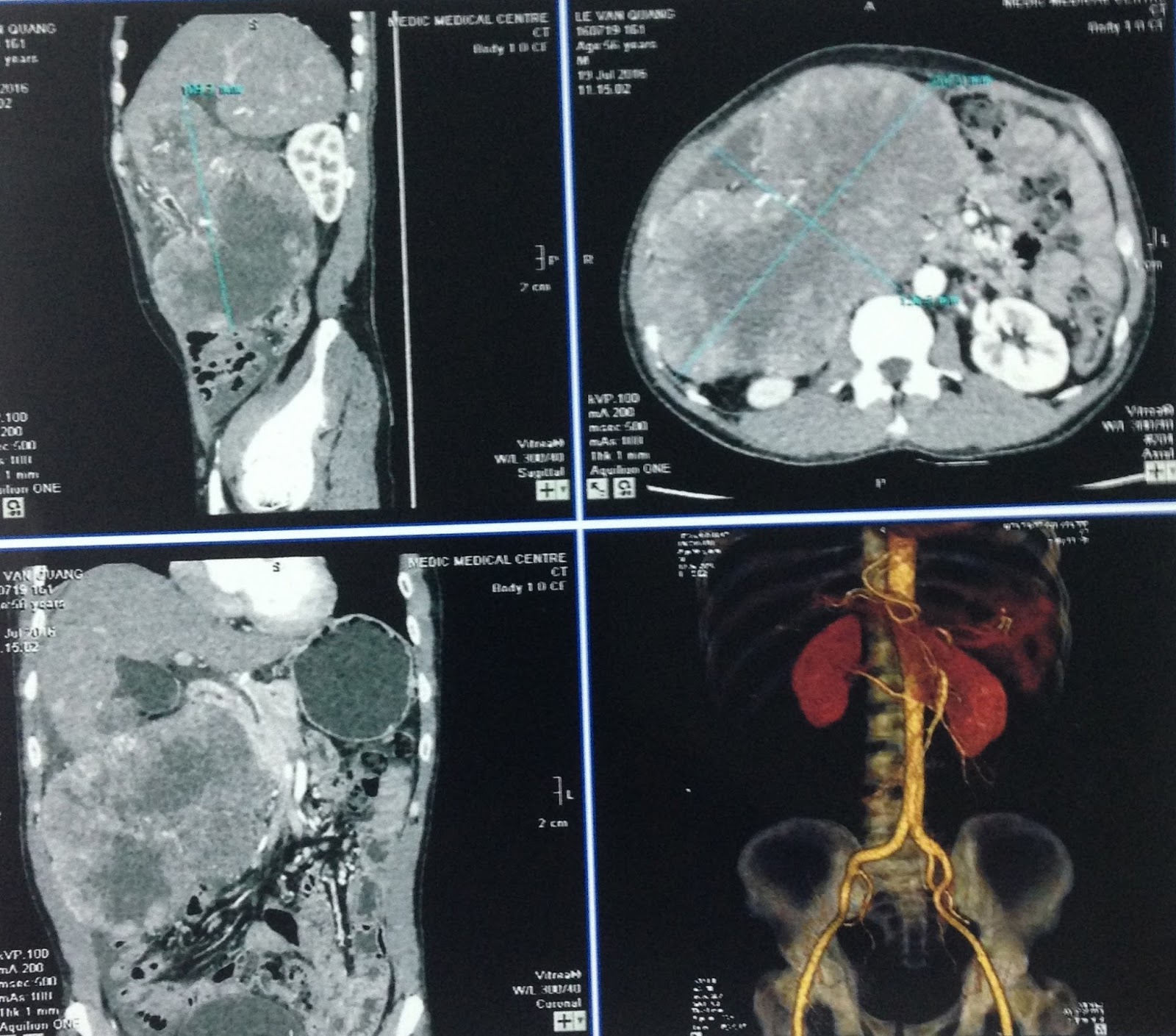
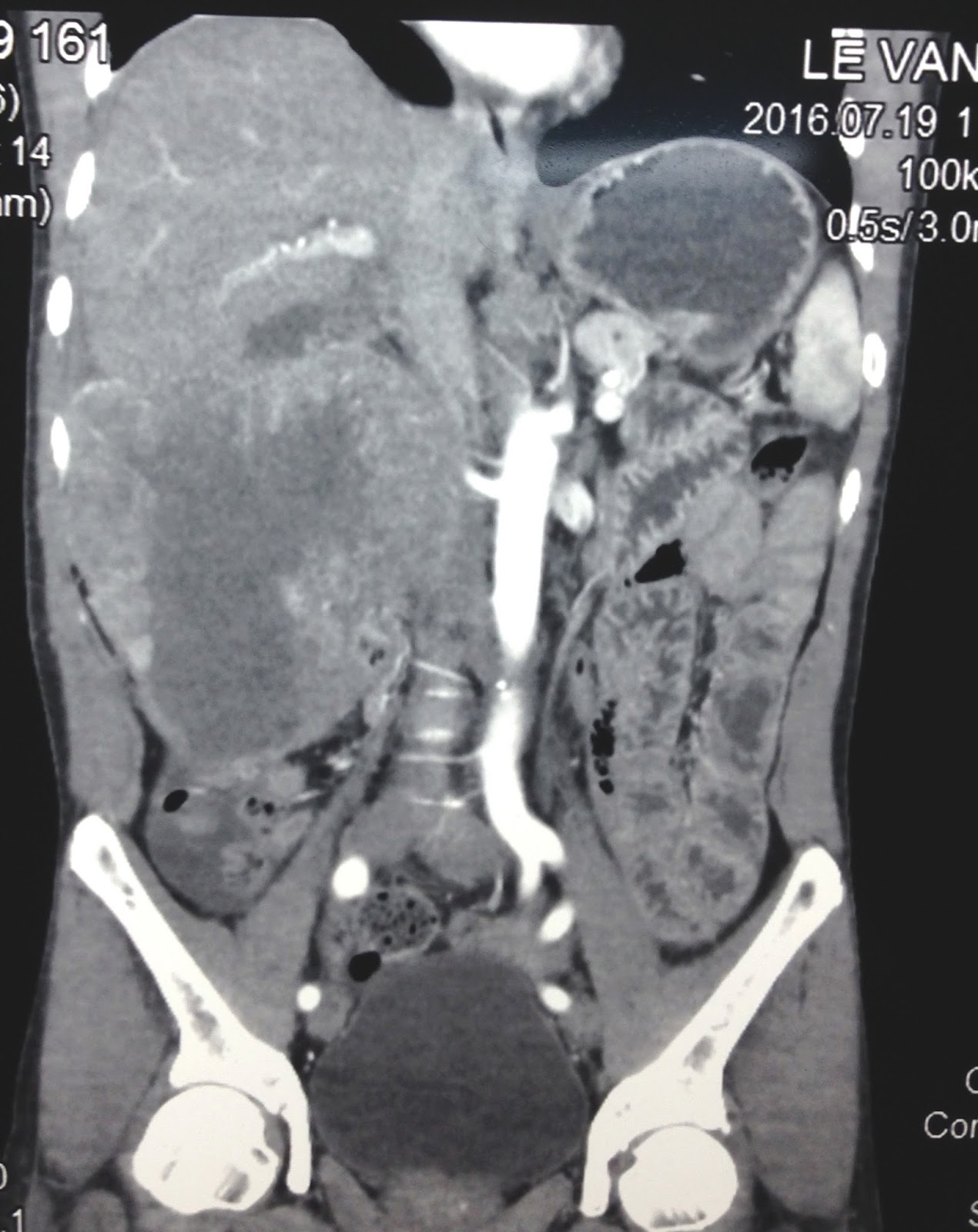
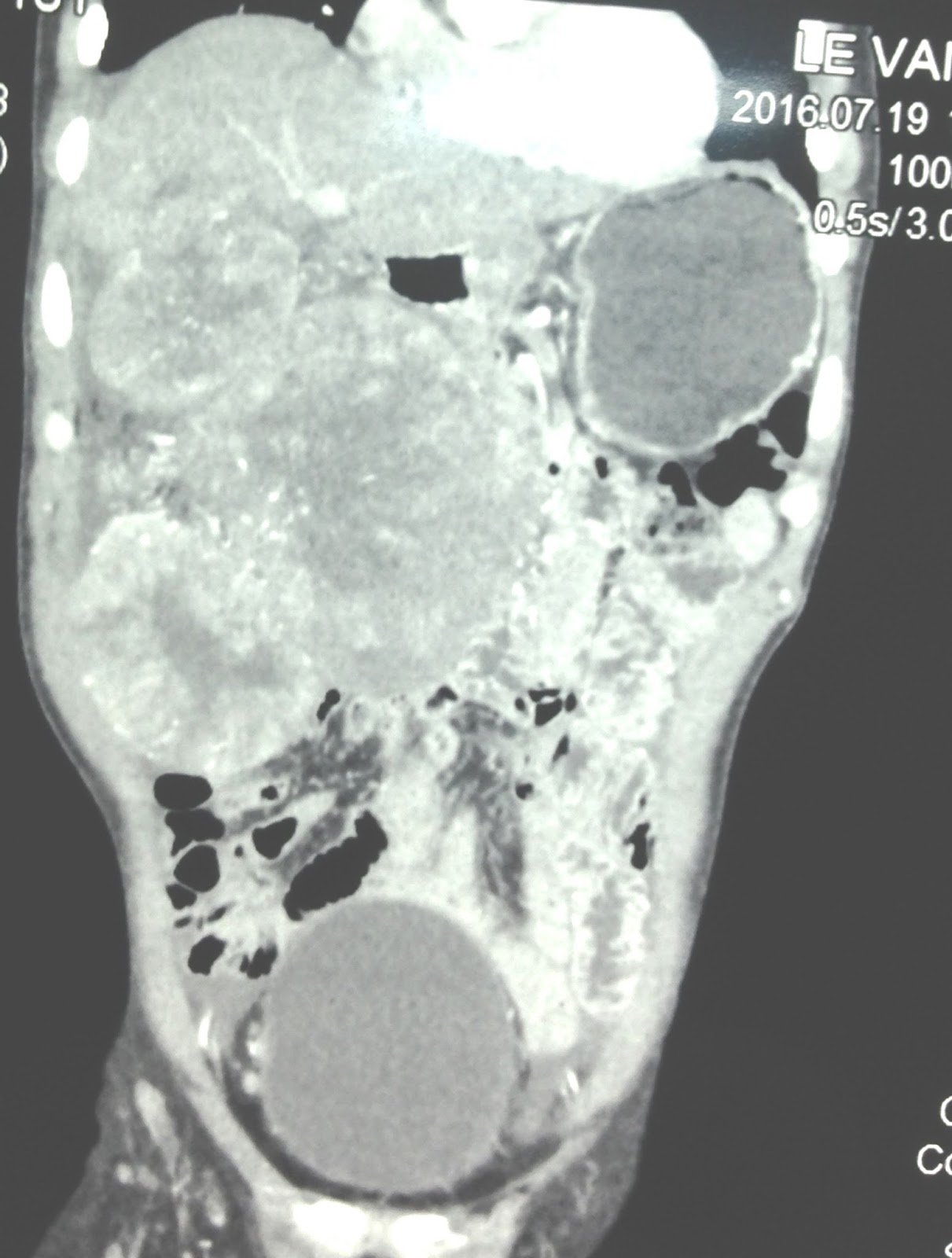
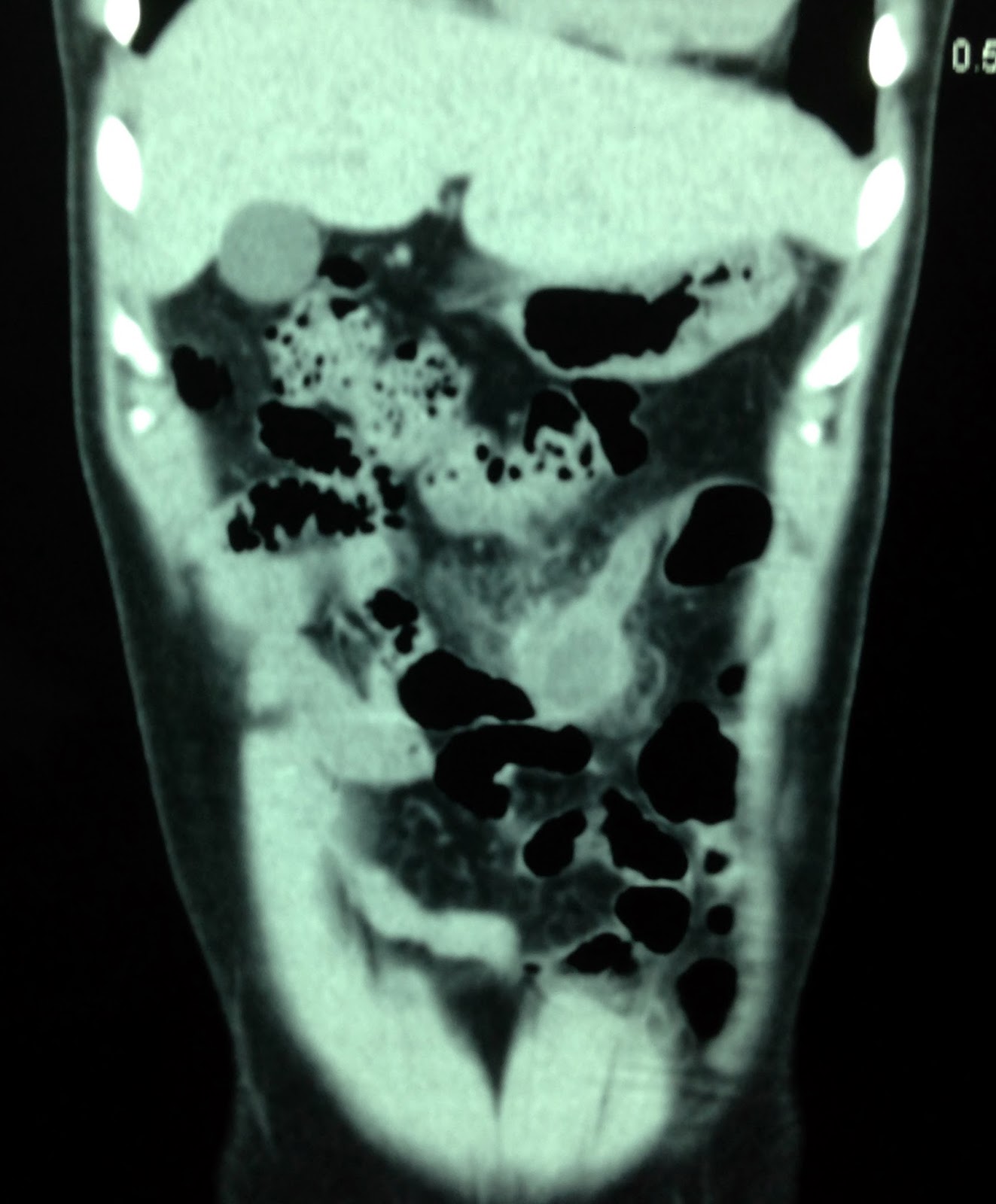
CT with CE:CT 1
non CE , CT2 CE, delay phase with central mass lower perfusion.


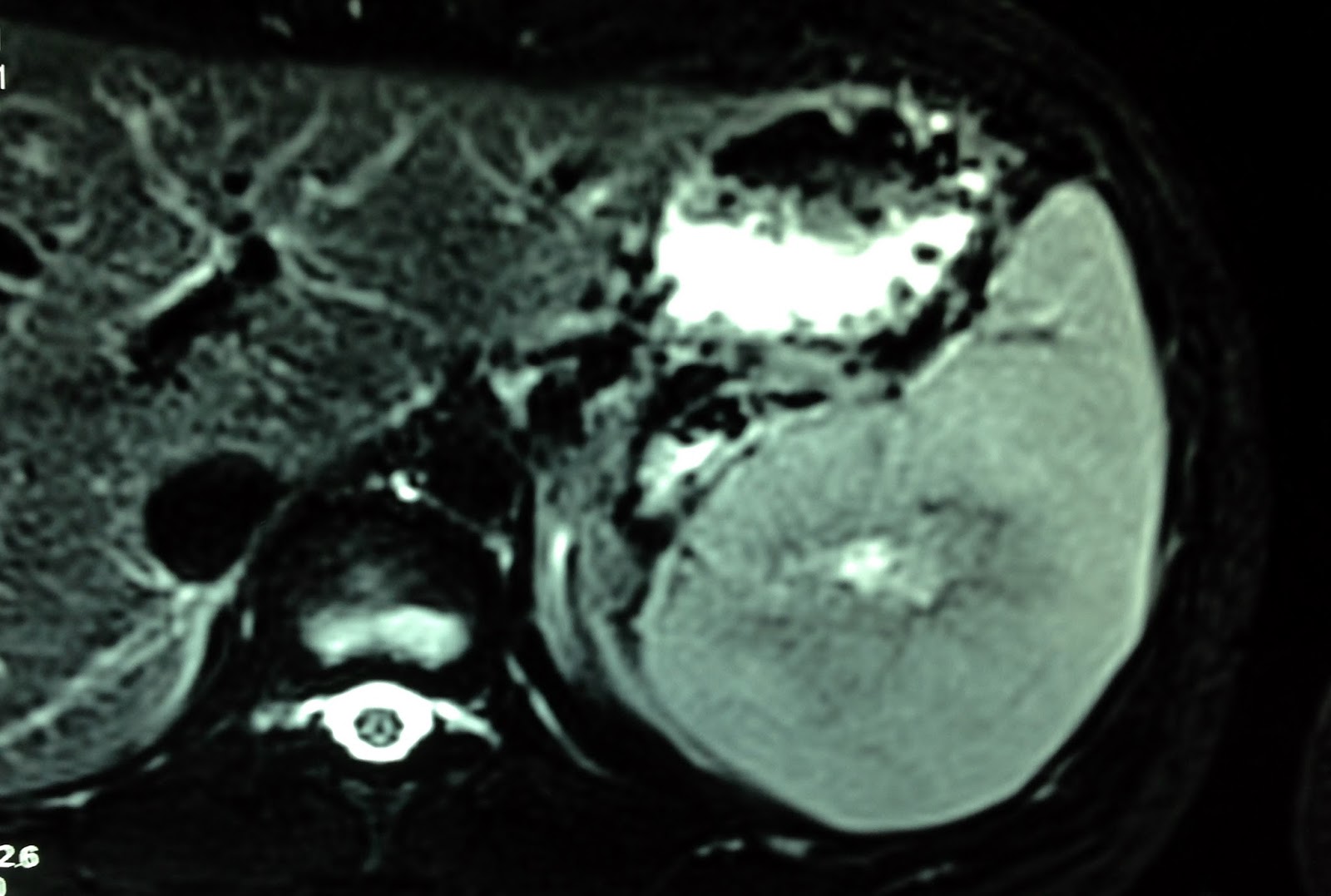
MRI with gado:
this tumor is well bordered, peripheral enhanced and central
hypoperfusion at the late phase.