A female 19 yo patient,
student, swelling and pain in the parotid glands about a week, not fever.
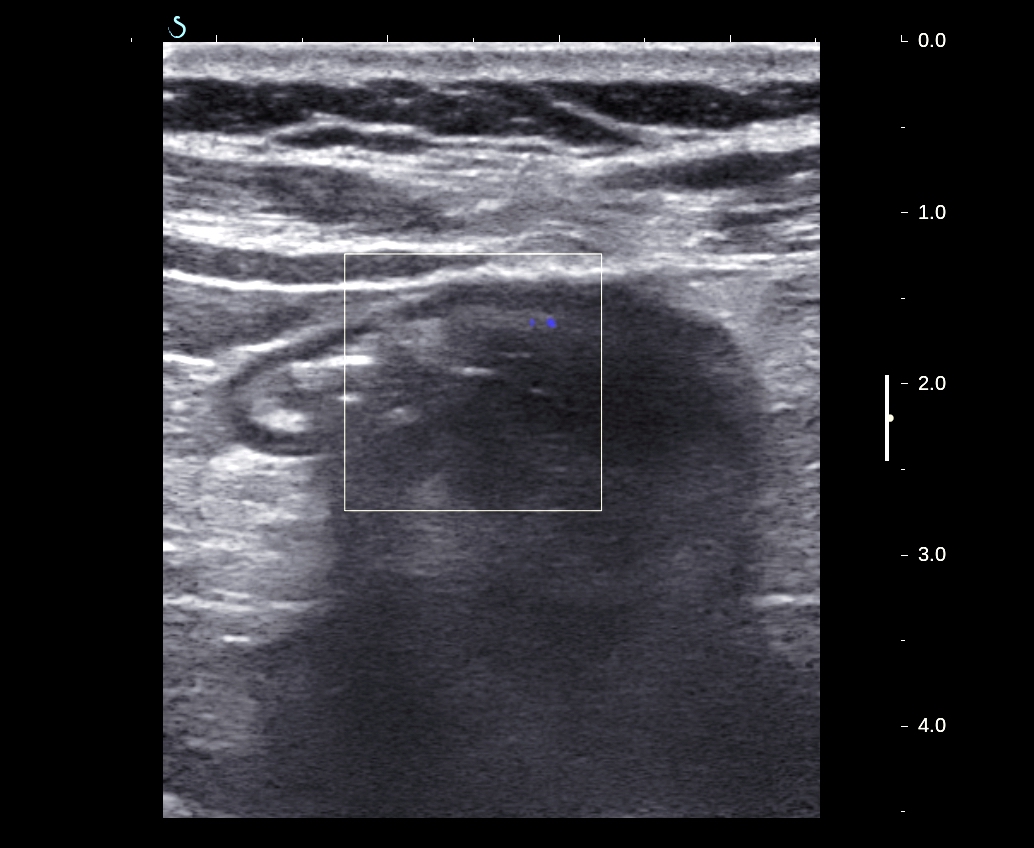
Ultrasonography showed
multiple structures within the parotid glands on 2 sides, hypoechoic,
well-defined, measuring approximately 5 - 12 mm, with the umbilical node. She
was diagnosed inflammation of the parotid glands and antibiotics for ten days (cephalosporin 3 and fluoroquinolon).
But parotid glands
swelling continuosly, ultrasound images with more nodules in the
parotid glands,and antibiotics for ten days again. In next follow-up visit parotid glands biopsy was
done, and result showed chronic salivary gland inflammation.
Patient was sent to
hospitalization Ho Chi Minh city in dentomaxillofacial center for 2 weeks of
antibiotics as Sjogren syndrome. Parotid
glands still swollen and had discharge
line to detect skin. And she returned to
MEDIC for parotid gland ultrasound.
Ultrasound image showed
multiple hypoechoic structures with fluid inside, well-defined, proliferative
vascular supplying, created road detect skin.
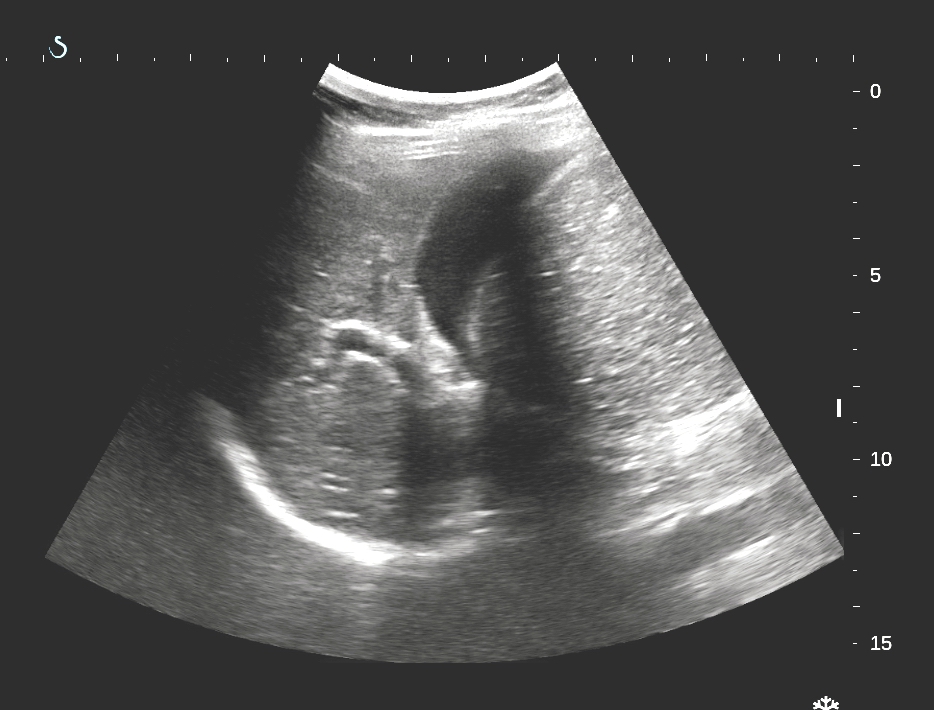
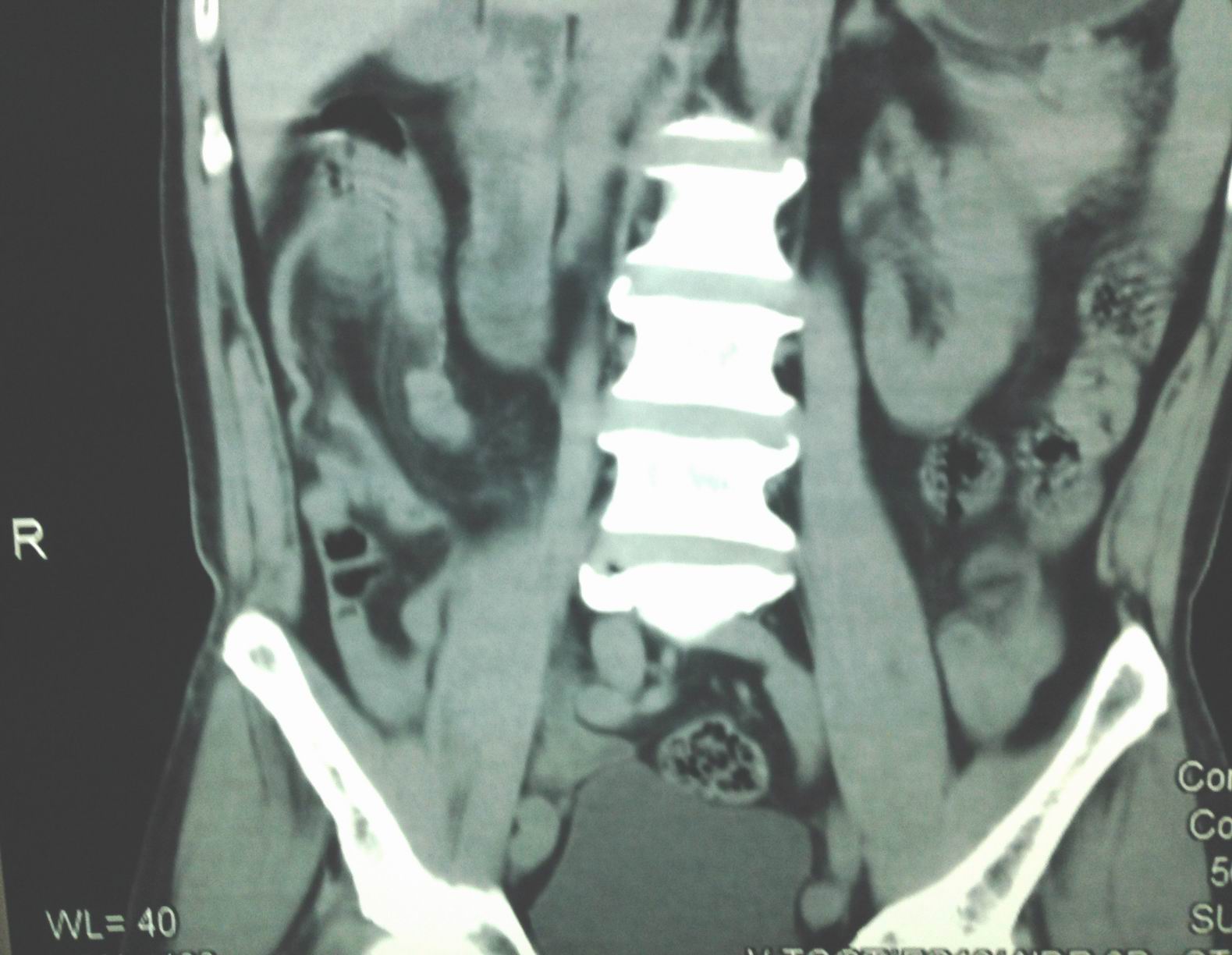
MSCT with CE showed
parotid gland hypertrophy, having multiple lesions with fluid density in the
central area.
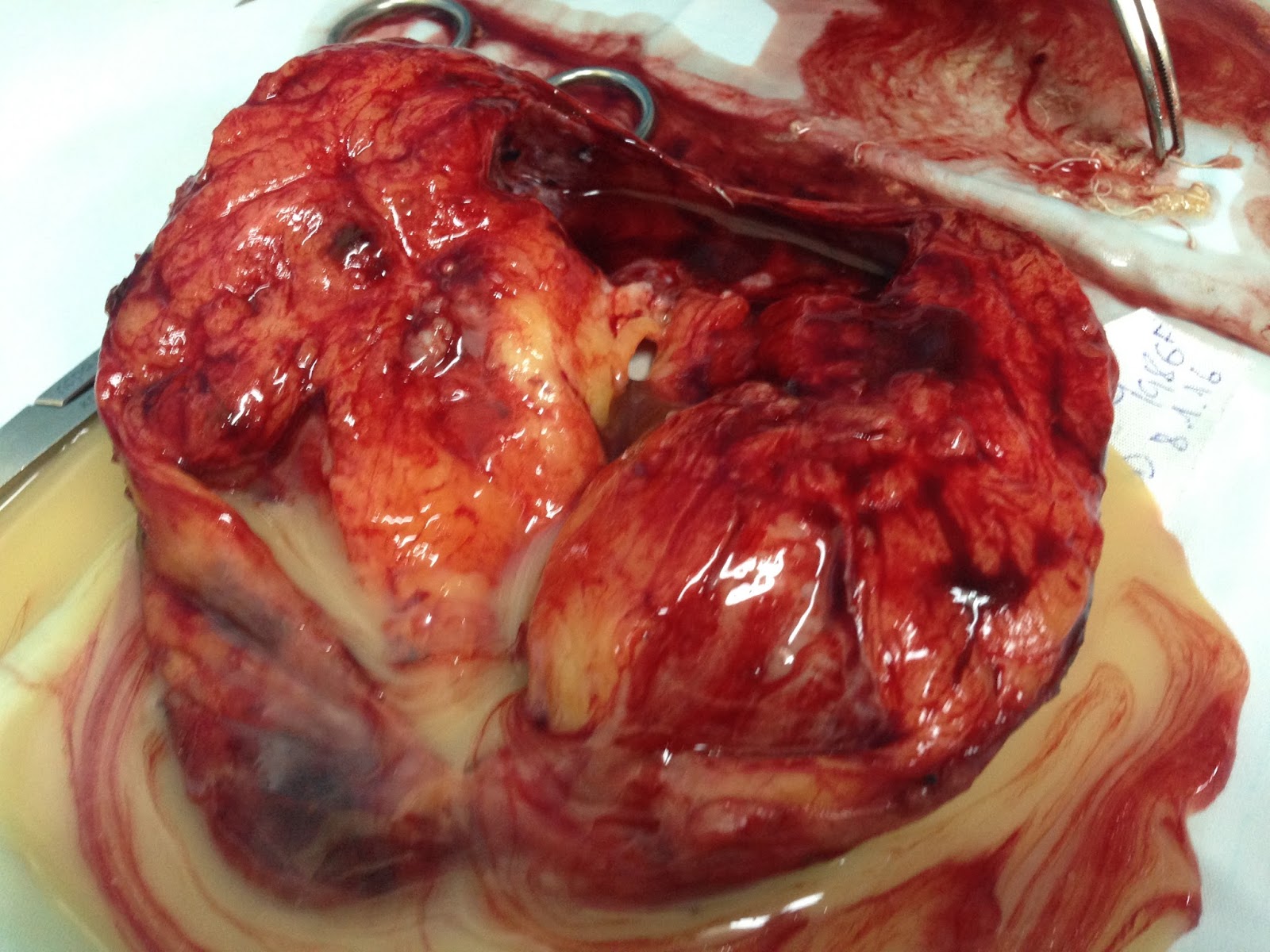
Parotid gland biopsy
showed salivary gland with Langhans great cells.
Parotid gland fluid examination showed high ADA and
PCR/ TB (+).