Woman 79 yo being
treated right kidney stone. 3 years ago, with
ultrasound of abdomen in black
and white images detected a stone with size 1 cm (US 1, US 2
longitudinal scan and crossed section of right kidney).


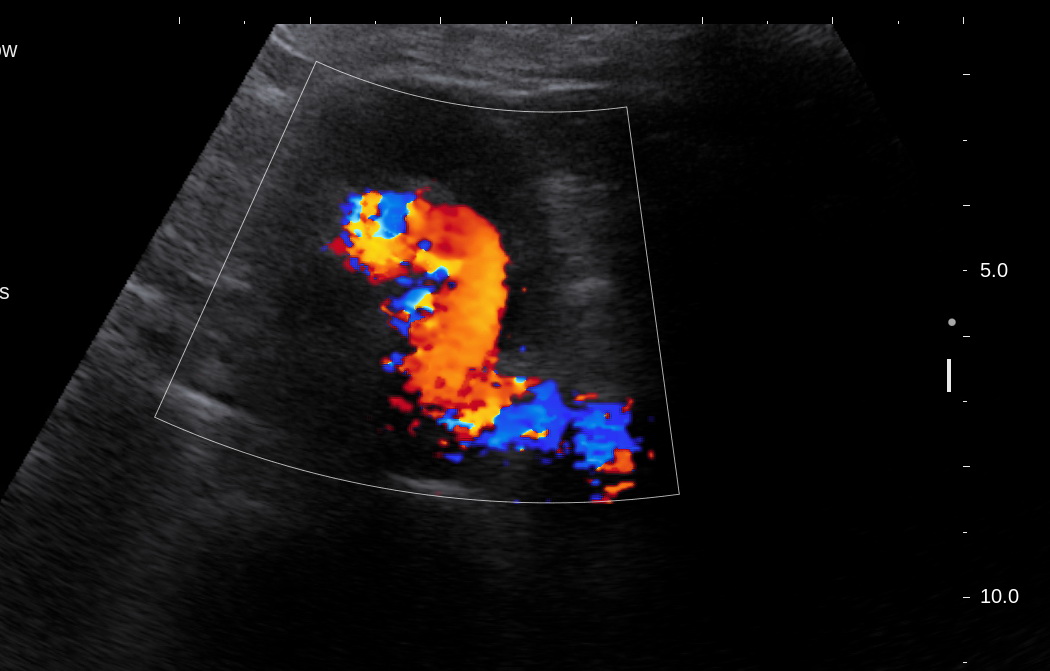
On color Doppler
it exists an AVM with calcification ( US 3, US 4).

MSCT with CE of abdomen for sure AVM of right kidney (CT 1,CT 2, CT 3,
CT 4, CT 5) , radiologist reported at CT 3 image one
mass at pelvis like sigmoid colon tumor.





Coloendoscopy confirmed that rectum tumor # 16 cm, high from anus.

Biopsy on the way
(endoscopic image)
MRI preop takes
staging of rectum cancer T4 N1 Mx.



Conclusion: Abdomen CT
for diagnosing AVM of right kidney detected incidentally a rectum
cancer on AVM and stone kidney patient.

MACROSCOPIC REPORT IS ADENOCARCINOMA OF RECTUM.

SUMMARY = CTA IS THE BEST DIAGNOSING MODALITY for RENAL AVM at THE SAME TIME OF INCIDENTAL DIAGNOSING FOR RECTUM CANCER WHICH WAS MISTAKED BY ULTRASOUND.