Woman 44 yo, 3 years ago after removing a small skin tumor [2005] at the left back with the result of skin hemangioma, this site is growing another
black tumor foto), size
arround 3 cm.

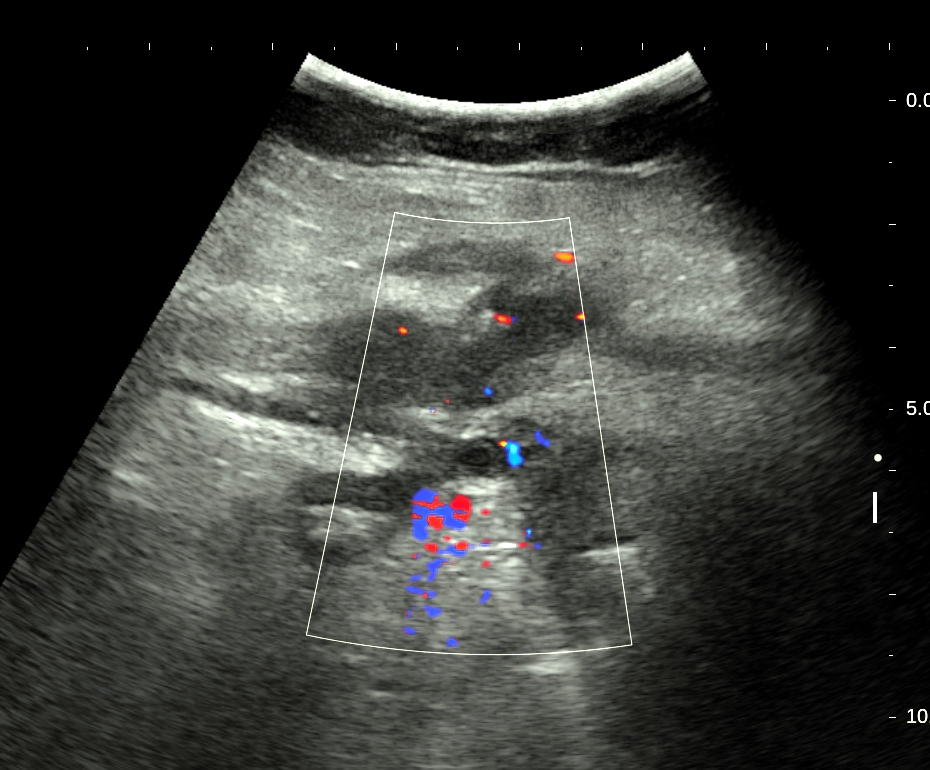
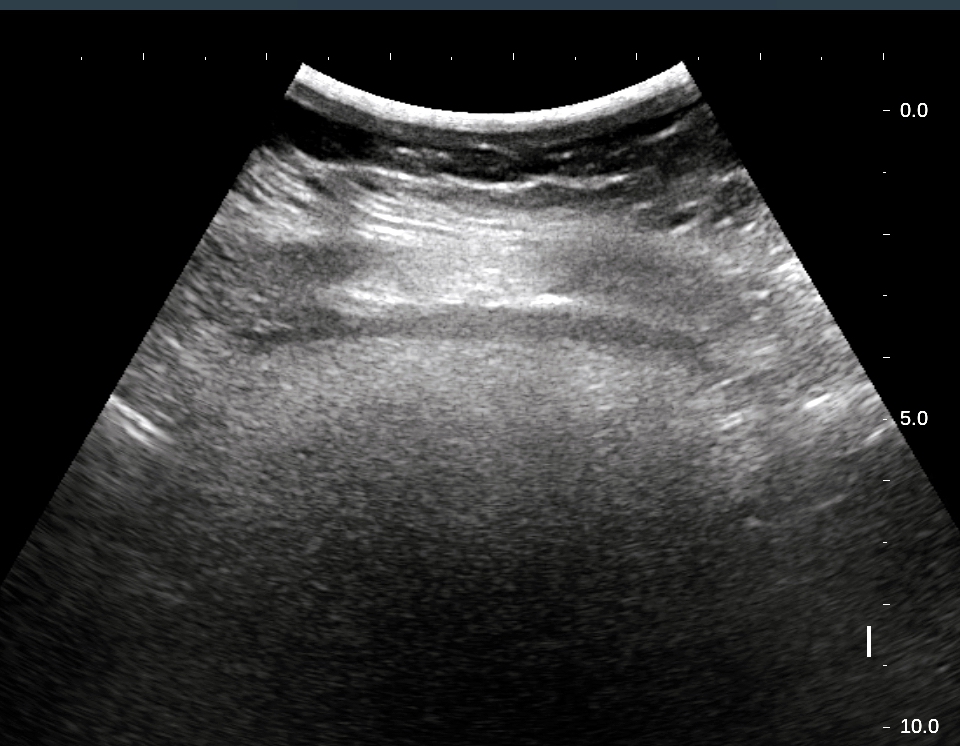
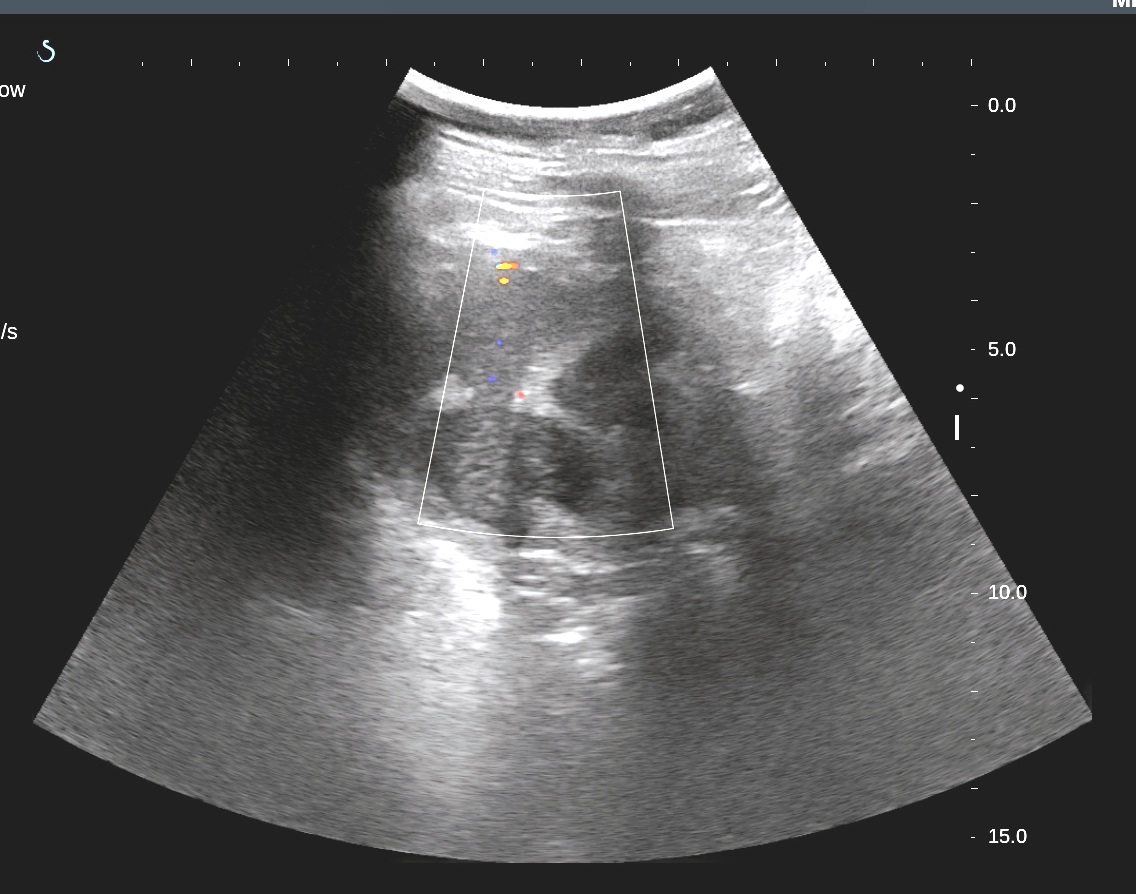
Ultrasound of skin
tumor= US 1: solid
tumor, inhomogenous structure, located subcutaneous to superficial
muscular fascia.

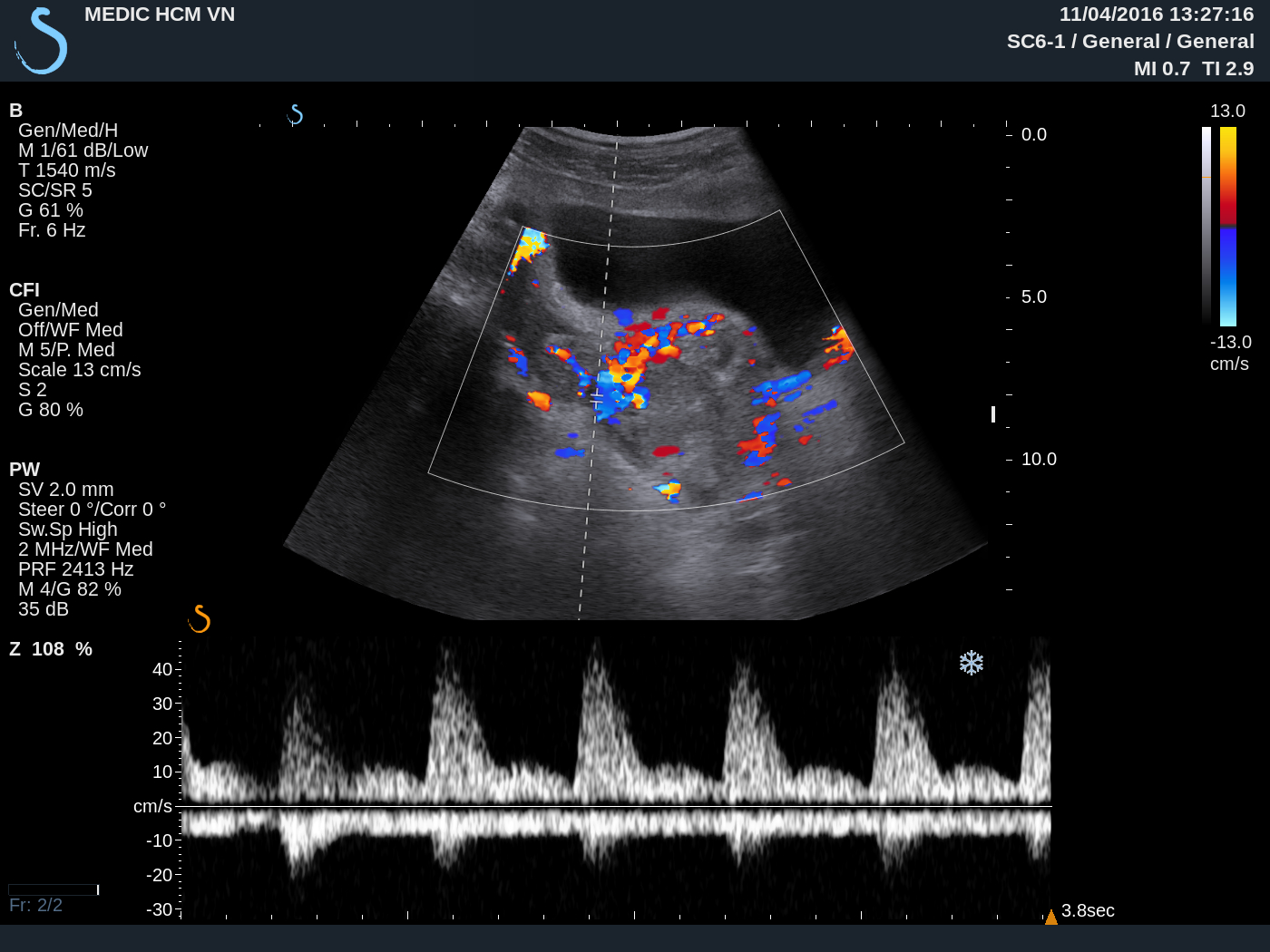
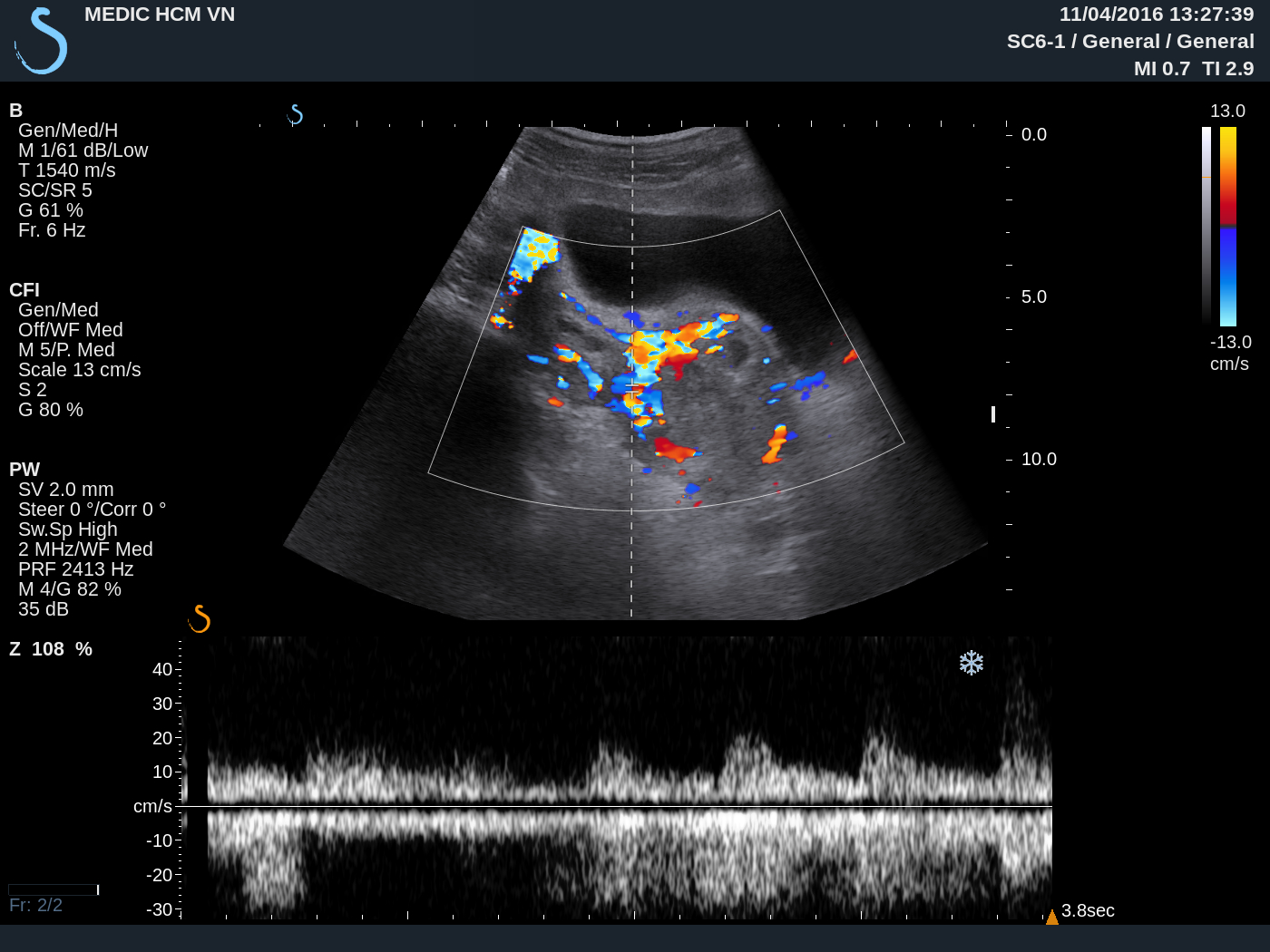
US 2: very high vascular structure of this tumor
on
color Doppler.

US 3: Power Doppler very high flow, lower RI of artery in tumor.

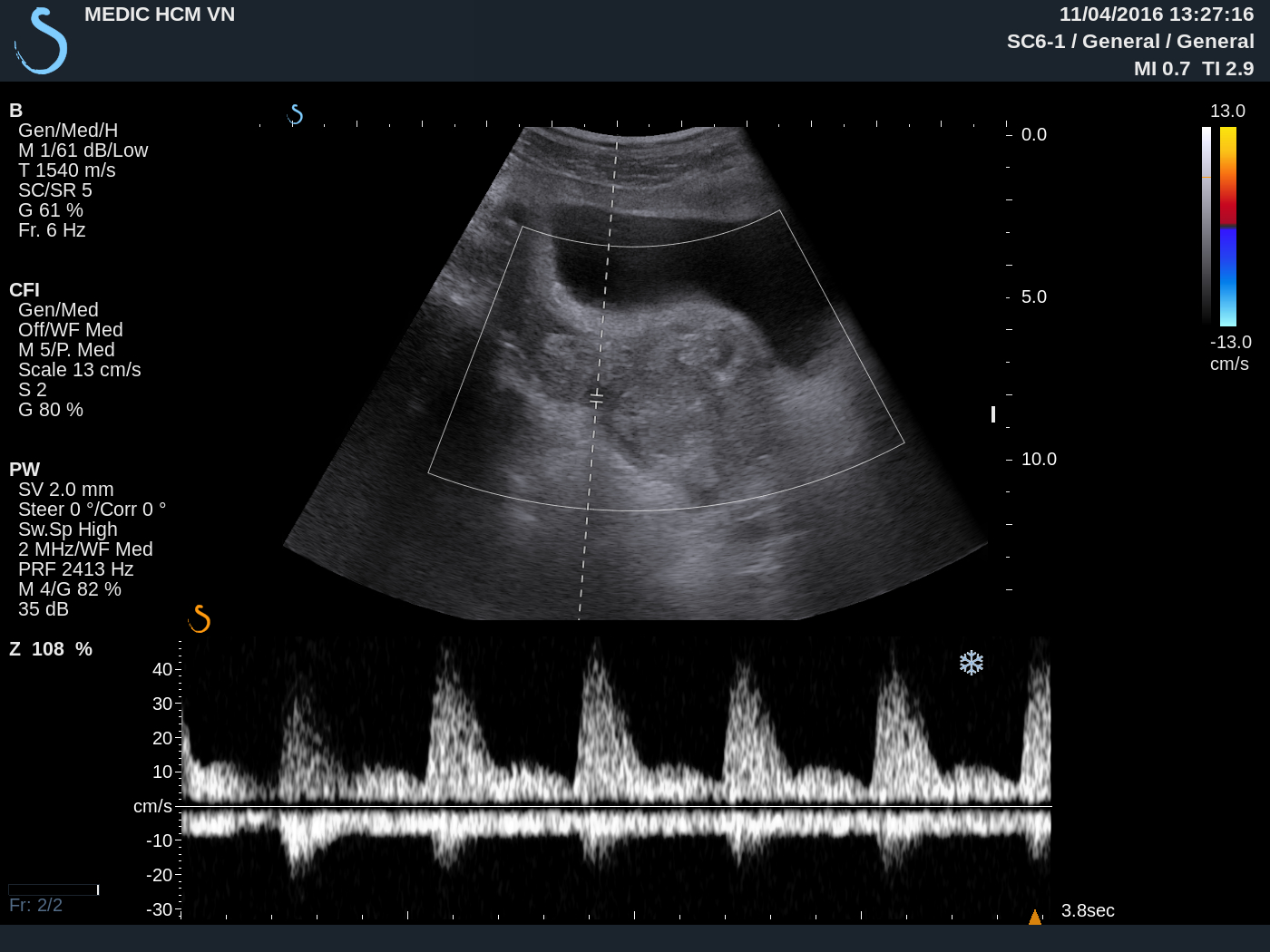
US 4: PW Doppler
of the main
artery supply of this tumor= very high flow, high PI.

What is your diagnosis for this cases? It is a recurrent black
tumor.