Woman 60 yo being treated
lymphoma large B cell
stage IV by chemotherapy for 5 months.
One week ago she herself detected many subcutaneous nodules
palpable at forearm right and left, neck and right
parotid area, no painful.
ULTRASOUND=
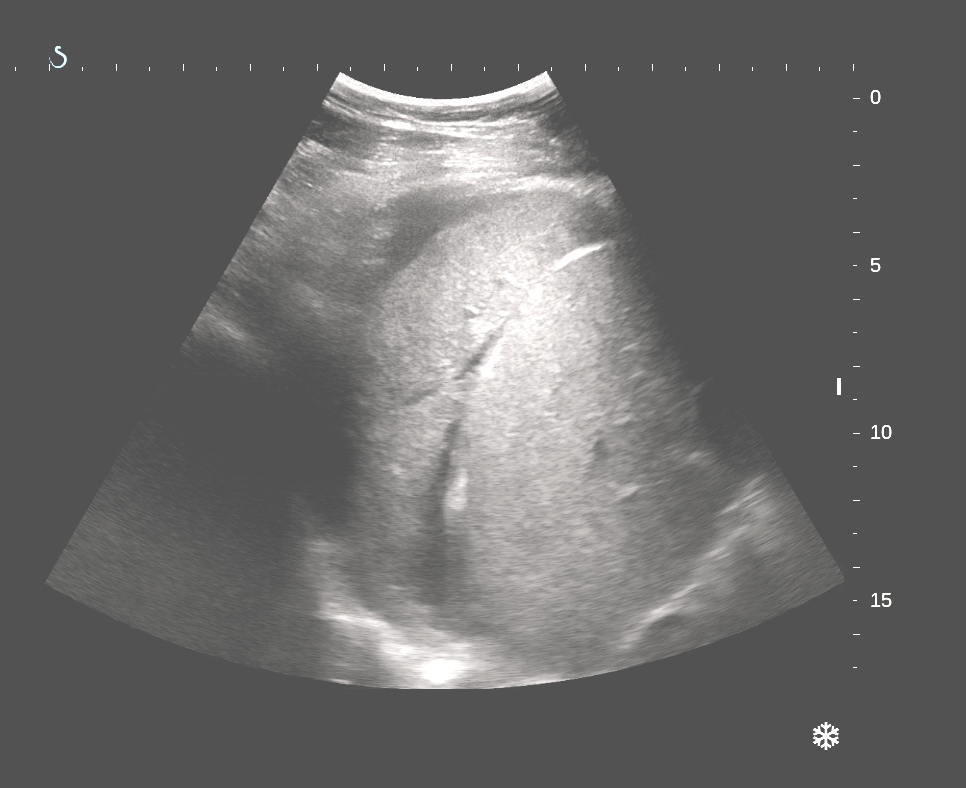
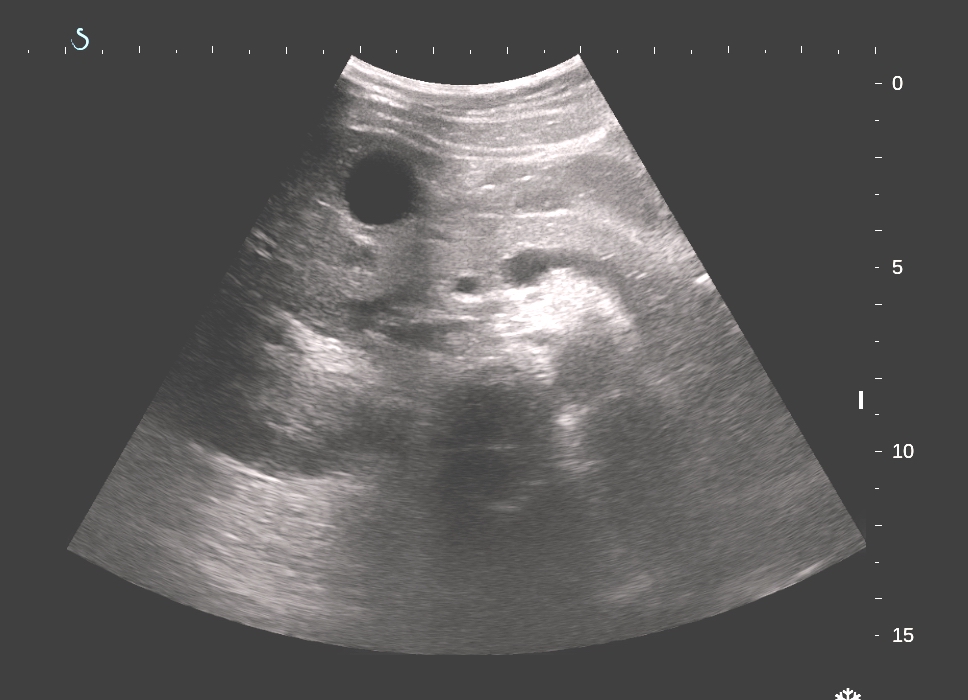
US 1=tumor intramuscular right
forearm, round border, very low echo density.

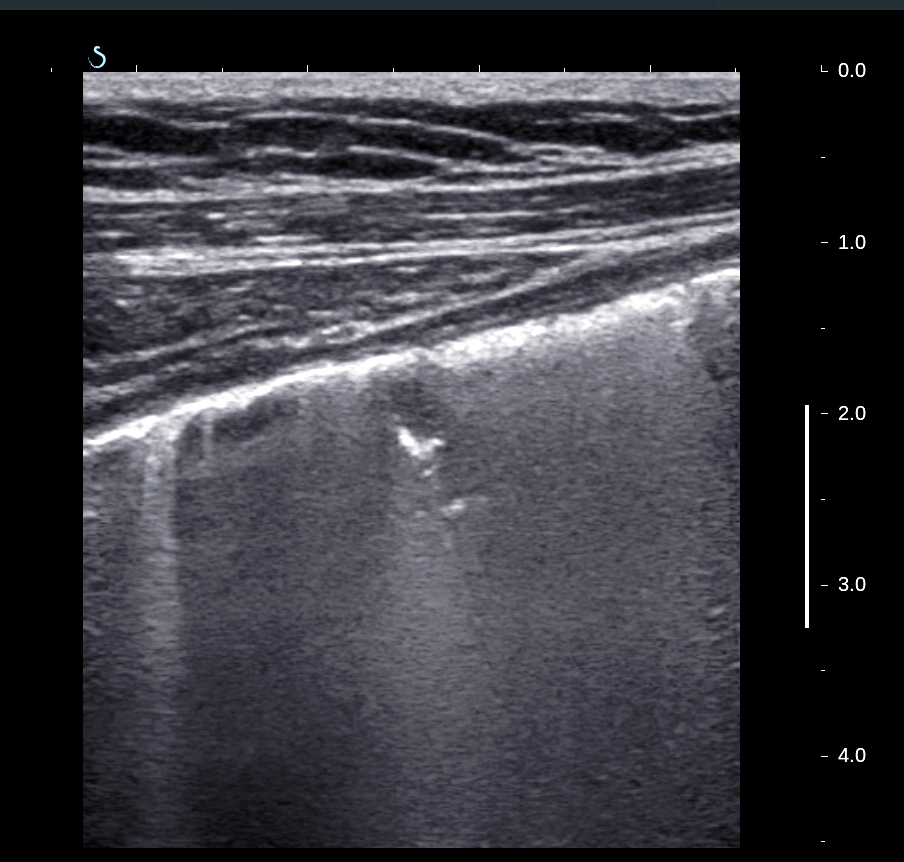
US 2=cross-section, lesion
at forearm.

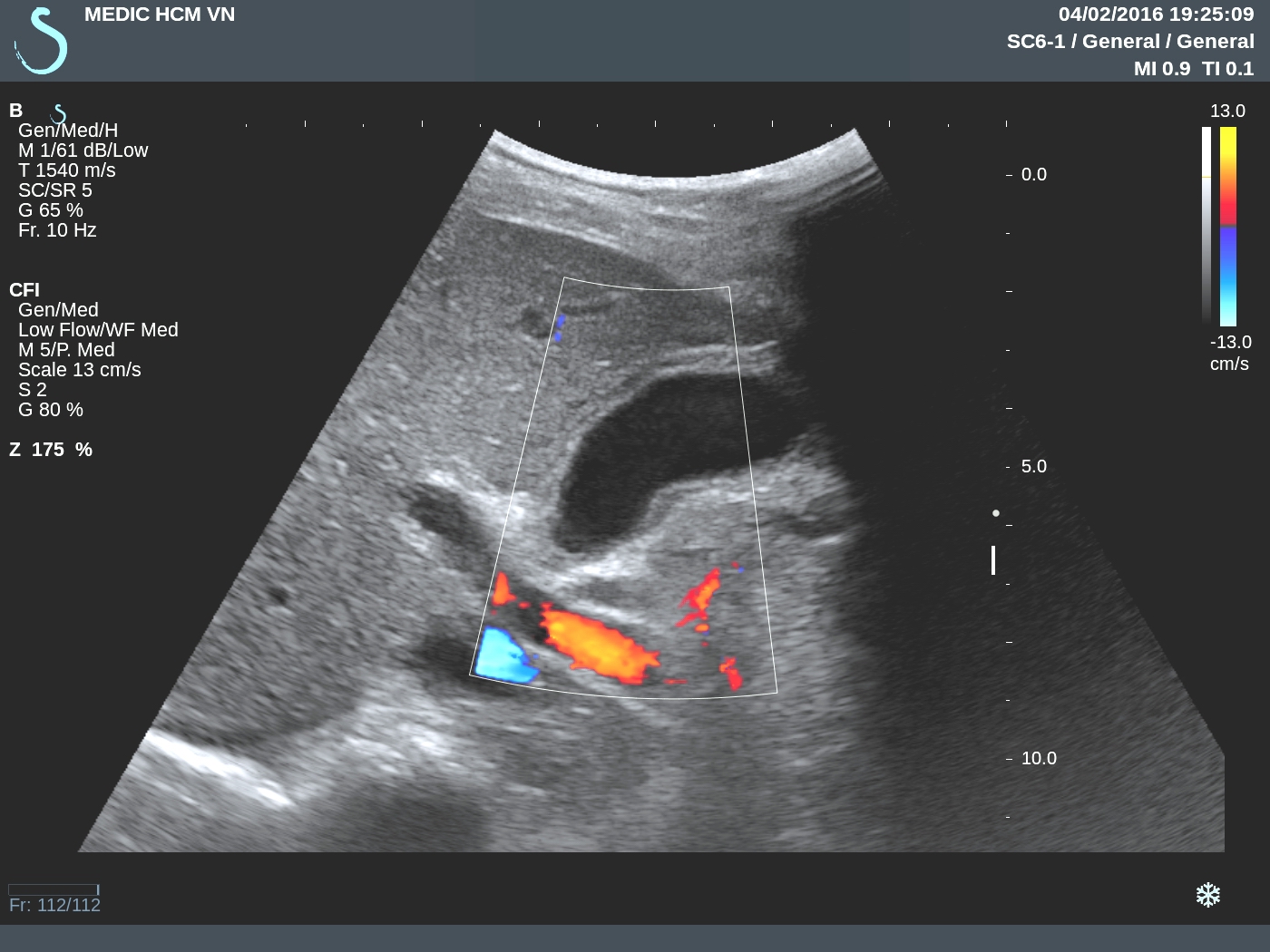
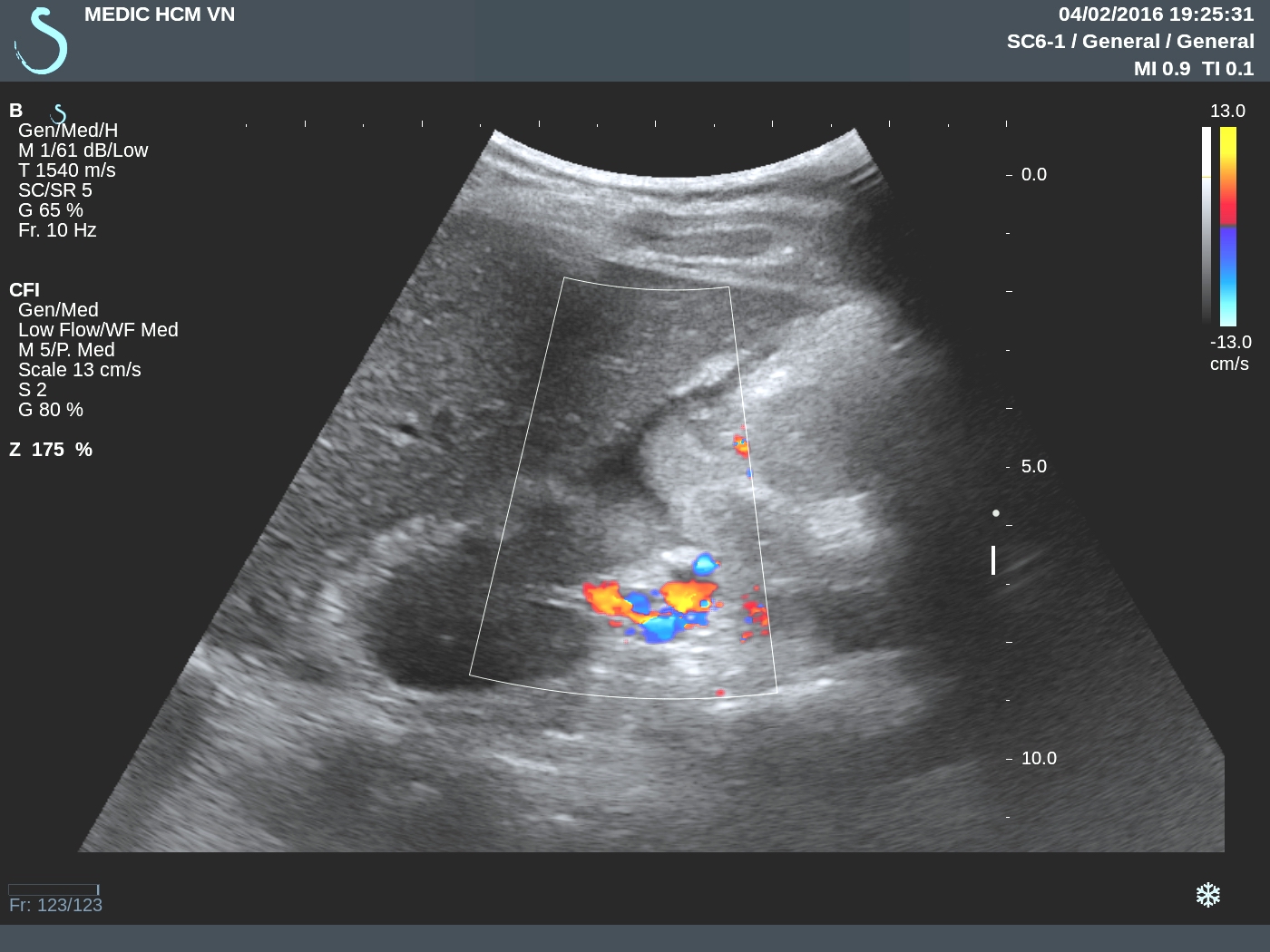
US 3=CDI Doppler vascular
structure of this
mass, hypervascular.

US 4=longitudinal scanning with CDI.

US 5=CDI with PW, RI = 0,70.

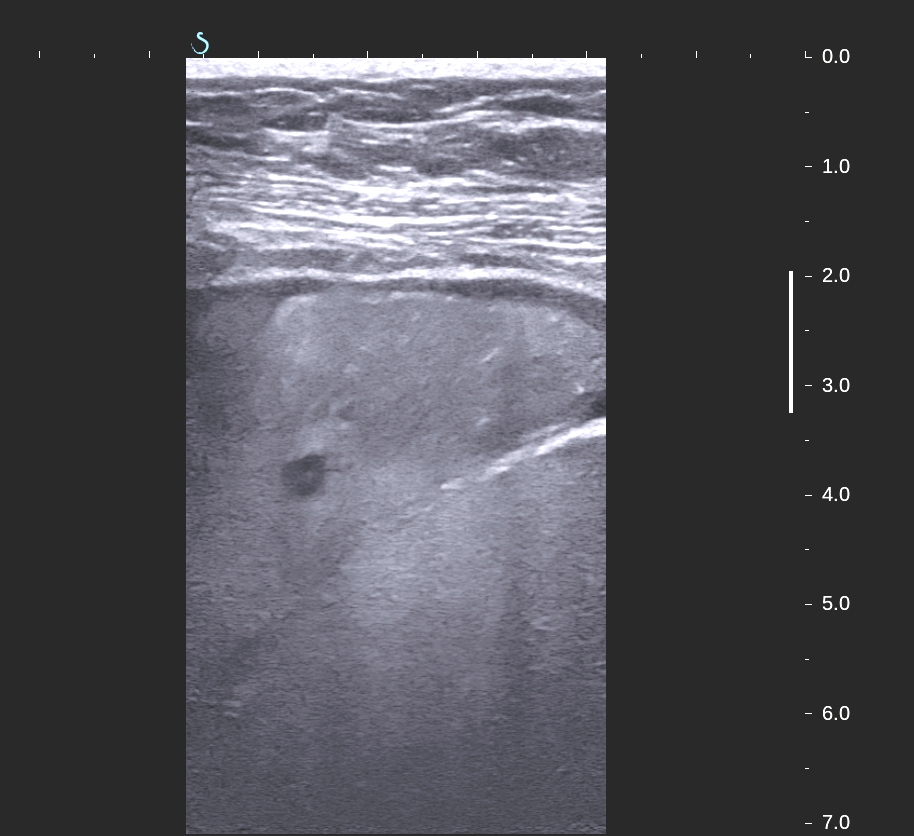
US 6 = small intramuscular nodule
at posterior of neck.

US 7= SWE of mass in right
parotid.

Do you thing it is lymphoma
in muscle?
Biopsy of this mass is large B cell lymphoma, same as result pre-treatment.

Conclusion: LYMPHOMA LARGE B CELL AT THE DIFFUSE STAGE CAN MAKE MULTIPLE NODULES IN MUSCLES.
Reference:

Reference: